

Mid-wall striae fibrosis predicts heart failure admission, composite heart failure events, and life-threatening arrhythmias in dilated cardiomyopathy
- PMID: 35110630
- PMCID: PMC8810767
- DOI: 10.1038/s41598-022-05790-y
Mid-wall striae fibrosis predicts heart failure admission, composite heart failure events, and life-threatening arrhythmias in dilated cardiomyopathy
Abstract
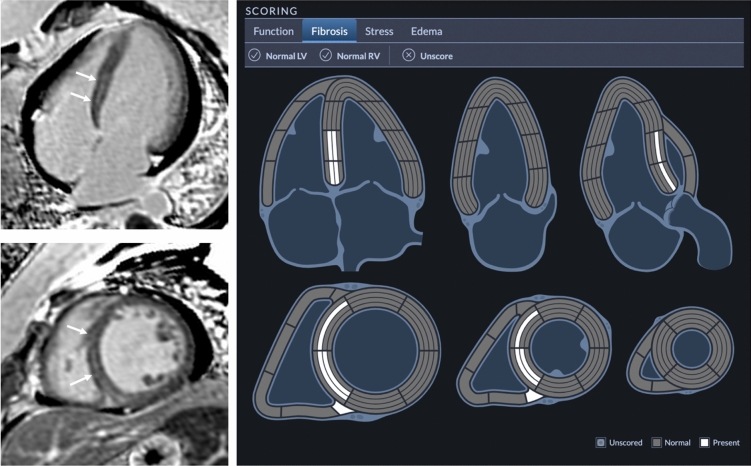
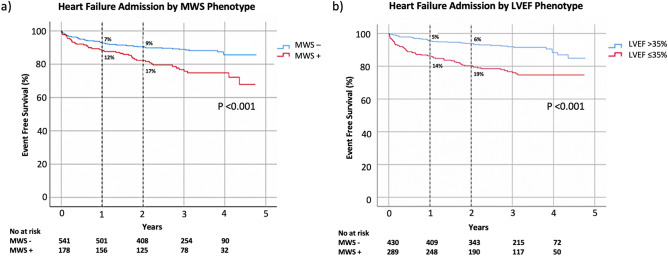
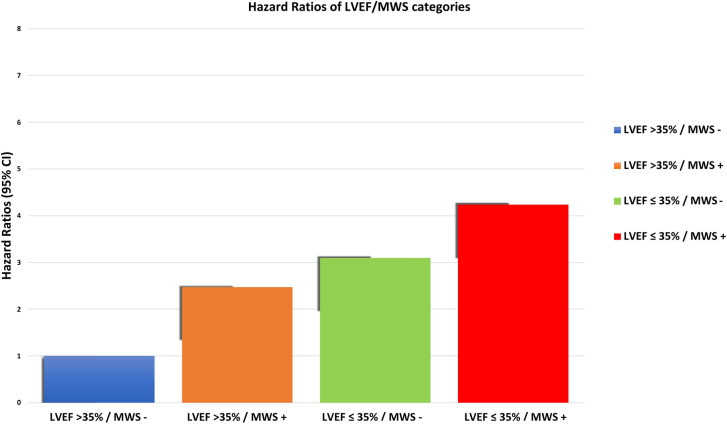
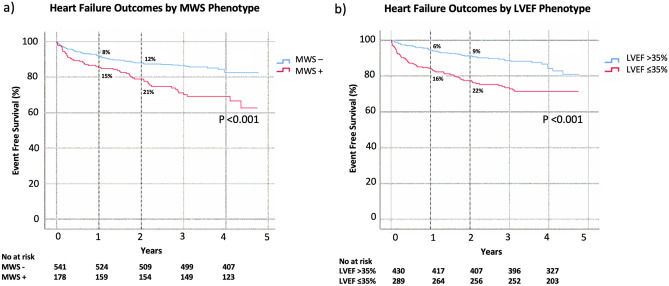
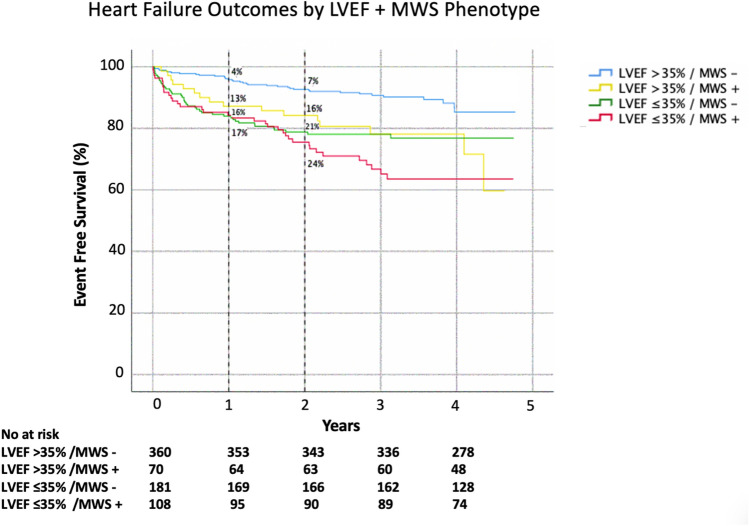
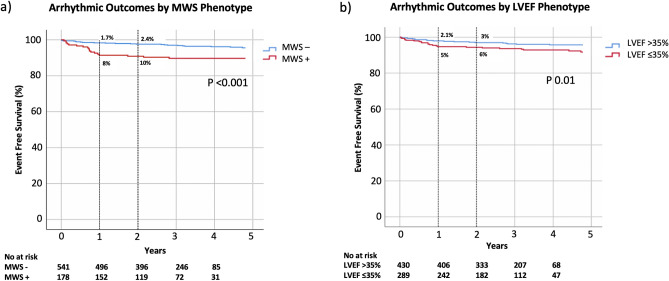
Heart failure (HF) admission is a dominant contributor to morbidity and healthcare costs in dilated cardiomyopathy (DCM). Mid-wall striae (MWS) fibrosis by late gadolinium enhancement (LGE) imaging has been associated with elevated arrhythmia risk. However, its capacity to predict HF-specific outcomes is poorly defined. We investigated its role to predict HF admission and relevant secondary outcomes in a large cohort of DCM patients. 719 patients referred for LGE MRI assessment of DCM were enrolled and followed for clinical events. Standardized image analyses and interpretations were conducted inclusive of coding the presence and patterns of fibrosis observed by LGE imaging. The primary clinical outcome was hospital admission for decompensated HF. Secondary heart failure and arrhythmic composite endpoints were also studied. Median age was 57 (IQR 47-65) years and median LVEF 40% (IQR 29-47%). Any fibrosis was observed in 228 patients (32%) with MWS fibrosis pattern present in 178 (25%). At a median follow up of 1044 days, 104 (15%) patients experienced the primary outcome, and 127 (18%) the secondary outcome. MWS was associated with a 2.14-fold risk of the primary outcome, 2.15-fold risk of the secondary HF outcome, and 2.23-fold risk of the secondary arrhythmic outcome. Multivariable analysis adjusting for all relevant covariates, inclusive of LVEF, showed patients with MWS fibrosis to experience a 1.65-fold increased risk (95% CI 1.11-2.47) of HF admission and 1-year event rate of 12% versus 7% without this phenotypic marker. Similar findings were observed for the secondary outcomes. Patients with LVEF > 35% plus MWS fibrosis experienced similar event rates to those with LVEF ≤ 35%. MWS fibrosis is a powerful and independent predictor of clinical outcomes in patients with DCM, identifying patients with LVEF > 35% who experience similar event rates to those with LVEF below this conventionally employed high-risk phenotype threshold.
© 2022. The Author(s).
Conflict of interest statement
Dr James White is a shareholder of Cohesic Inc and has received research funding from Siemens Healthineers. The remaining authors have nothing to disclose
Figures


Similar articles
-
Right ventricular insertion site fibrosis in a dilated cardiomyopathy referral population: phenotypic associations and value for the prediction of heart failure admission or death.J Cardiovasc Magn Reson. 2021 Jun 17;23(1):79. doi: 10.1186/s12968-021-00761-0. J Cardiovasc Magn Reson. 2021. PMID: 34134712 Free PMC article.
-
Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy.JAMA. 2013 Mar 6;309(9):896-908. doi: 10.1001/jama.2013.1363. JAMA. 2013. PMID: 23462786
-
Prognostic Value of Late Gadolinium Enhancement for the Prediction of Cardiovascular Outcomes in Dilated Cardiomyopathy: An International, Multi-Institutional Study of the MINICOR Group.Circ Cardiovasc Imaging. 2020 Apr;13(4):e010105. doi: 10.1161/CIRCIMAGING.119.010105. Epub 2020 Apr 21. Circ Cardiovasc Imaging. 2020. PMID: 32312112
-
Late Gadolinium Enhancement and the Risk for Ventricular Arrhythmias or Sudden Death in Dilated Cardiomyopathy: Systematic Review and Meta-Analysis.JACC Heart Fail. 2017 Jan;5(1):28-38. doi: 10.1016/j.jchf.2016.09.017. Epub 2016 Dec 21. JACC Heart Fail. 2017. PMID: 28017348 Review.
-
The Prognostic Value of Late Gadolinium-Enhanced Cardiac Magnetic Resonance Imaging in Nonischemic Dilated Cardiomyopathy: A Review and Meta-Analysis.JACC Cardiovasc Imaging. 2018 Sep;11(9):1274-1284. doi: 10.1016/j.jcmg.2018.03.006. Epub 2018 Apr 18. JACC Cardiovasc Imaging. 2018. PMID: 29680351 Review.
Cited by
-
Marfan Syndrome beyond Aortic Root-Phenotyping Using Cardiovascular Magnetic Resonance Imaging and Clinical Implications.Medicina (Kaunas). 2023 May 14;59(5):942. doi: 10.3390/medicina59050942. Medicina (Kaunas). 2023. PMID: 37241174 Free PMC article.
References
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, et al. Classification of the cardiomyopathies: A position statement from the European society of cardiology working group on myocardial and pericardial diseases. Eur Heart J. 2008;29(2):270–276. doi: 10.1093/eurheartj/ehm342. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
