

NK cells in the brain: implications for brain tumor development and therapy
- PMID: 35078713
- PMCID: PMC8882142
- DOI: 10.1016/j.molmed.2021.12.008
NK cells in the brain: implications for brain tumor development and therapy
Abstract
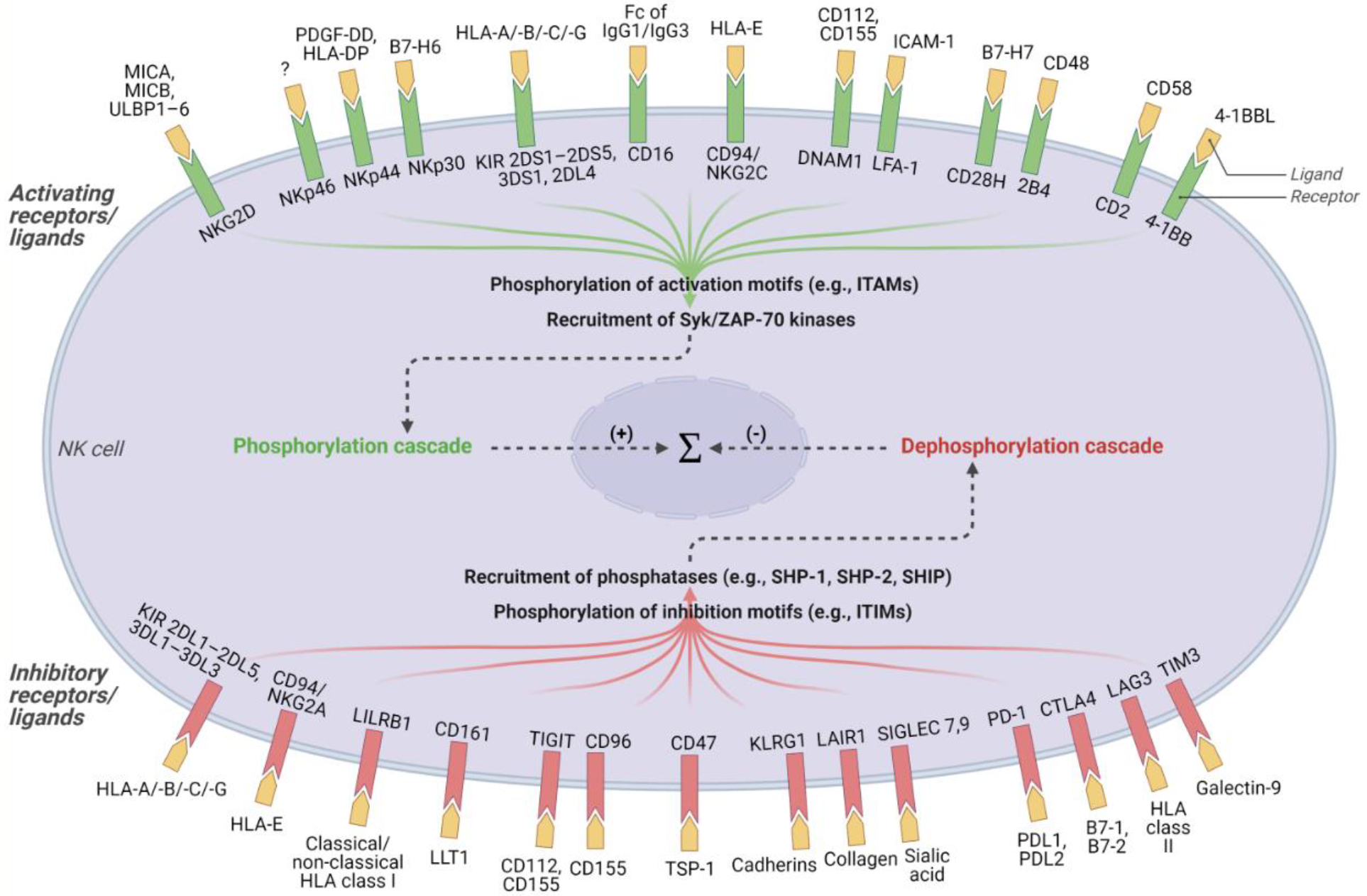
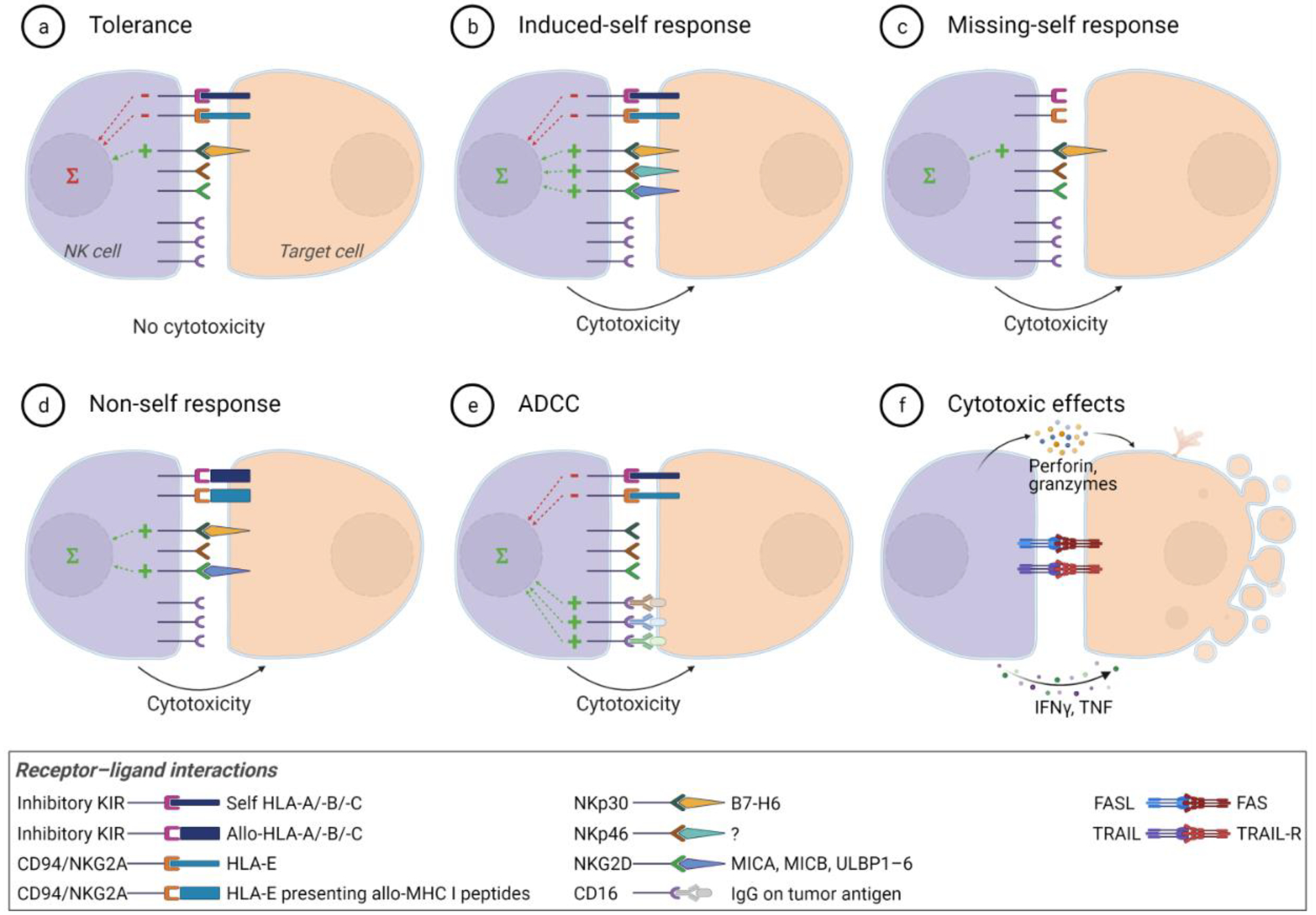
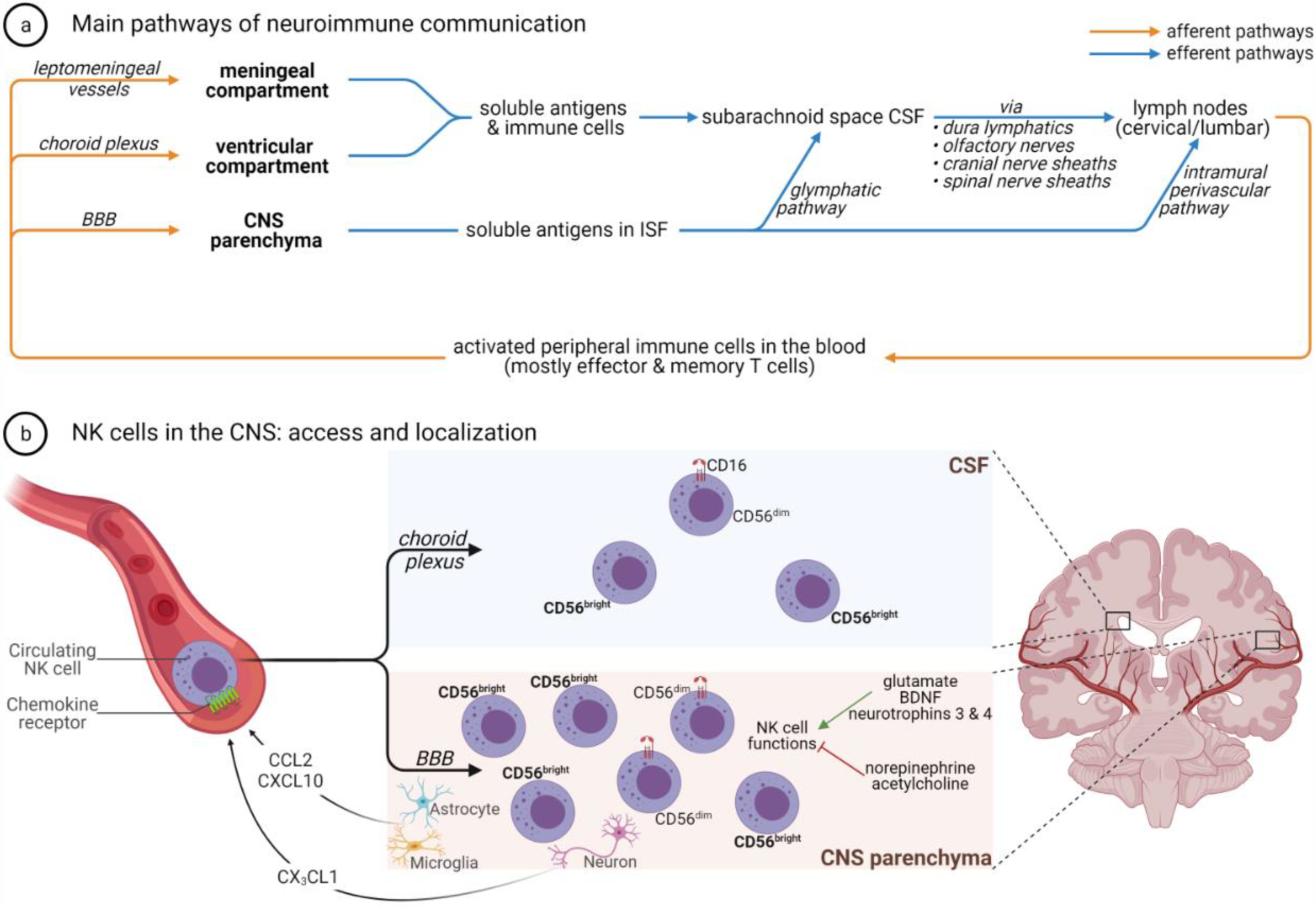
Natural killer (NK) cells are innate lymphoid cells with robust antitumor functions rendering them promising therapeutic tools against malignancies. Despite constituting a minor fraction of the immune cells infiltrating tumors in the brain, insights into their role in central nervous system (CNS) pathophysiology are emerging. The challenges posed by a profoundly immunosuppressive microenvironment as well as by tumor resistance mechanisms necessitate exploring avenues to enhance the therapeutic potential of NK cells in both primary and metastatic brain malignancies. In this review, we summarize the role of NK cells in the pathogenesis of tumors in the brain and discuss the avenues investigated to harness their anticancer effects against primary and metastatic CNS tumors, including sources of therapeutic NK cells, combinations with other treatments, and novel engineering approaches for augmenting their cytotoxicity. We also highlight relevant preclinical evidence and clinical trials of NK cell-based therapies.
Keywords: NK cells; glioblastoma; immunotherapy of the brain, clinical immunotherapy; neuroimmunology.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests K.S. owns equity in and is a member of the Board of Directors of AMASA Therapeutics, a company developing stem cell-based therapies for cancer. K.S.’s interests were reviewed and are managed by Brigham and Women’s Hospital and Partners HealthCare in accordance with their conflict of interest policies. The other authors declare that they have no competing interests.
Figures

Similar articles
-
CAR-Engineered NK Cells for the Treatment of Glioblastoma: Turning Innate Effectors Into Precision Tools for Cancer Immunotherapy.Front Immunol. 2019 Nov 14;10:2683. doi: 10.3389/fimmu.2019.02683. eCollection 2019. Front Immunol. 2019. PMID: 31798595 Free PMC article. Review.
-
Leveraging Natural Killer Cell Innate Immunity against Hematologic Malignancies: From Stem Cell Transplant to Adoptive Transfer and Beyond.Int J Mol Sci. 2022 Dec 22;24(1):204. doi: 10.3390/ijms24010204. Int J Mol Sci. 2022. PMID: 36613644 Free PMC article. Review.
-
Challenges to the broad application of allogeneic natural killer cell immunotherapy of cancer.Stem Cell Res Ther. 2022 Apr 12;13(1):165. doi: 10.1186/s13287-022-02769-4. Stem Cell Res Ther. 2022. PMID: 35414042 Free PMC article. Review.
-
Chimeric antigen receptor (CAR) natural killer (NK)-cell therapy: leveraging the power of innate immunity.Br J Haematol. 2021 Apr;193(2):216-230. doi: 10.1111/bjh.17186. Epub 2020 Nov 20. Br J Haematol. 2021. PMID: 33216984 Free PMC article. Review.
-
Targeting Natural Killer Cells for Tumor Immunotherapy.Front Immunol. 2020 Feb 19;11:60. doi: 10.3389/fimmu.2020.00060. eCollection 2020. Front Immunol. 2020. PMID: 32140153 Free PMC article. Review.
Cited by
-
NK Cells in Cancer: Mechanisms of Dysfunction and Therapeutic Potential.Int J Mol Sci. 2023 May 30;24(11):9521. doi: 10.3390/ijms24119521. Int J Mol Sci. 2023. PMID: 37298470 Free PMC article. Review.
-
Glioblastoma Therapy: Past, Present and Future.Int J Mol Sci. 2024 Feb 21;25(5):2529. doi: 10.3390/ijms25052529. Int J Mol Sci. 2024. PMID: 38473776 Free PMC article. Review.
-
Therapeutic effects against high-grade glioblastoma mediated by engineered induced neural stem cells combined with GD2-specific CAR-NK.Cell Oncol (Dordr). 2023 Dec;46(6):1747-1762. doi: 10.1007/s13402-023-00842-5. Epub 2023 Jul 7. Cell Oncol (Dordr). 2023. PMID: 37420122
-
Prospective Molecular Targets for Natural Killer Cell Immunotherapy against Glioblastoma Multiforme.Cells. 2024 Sep 17;13(18):1567. doi: 10.3390/cells13181567. Cells. 2024. PMID: 39329751 Free PMC article. Review.
-
Image-based assessment of natural killer cell activity against glioblastoma stem cells.FEBS Open Bio. 2024 Jun;14(6):1028-1034. doi: 10.1002/2211-5463.13818. Epub 2024 May 13. FEBS Open Bio. 2024. PMID: 38740554 Free PMC article.
References
-
- Shimasaki N et al. (2020) NK cells for cancer immunotherapy. Nat. Rev. Drug Discov 19, 200–218 - PubMed
-
- Abbas AK et al. (2018) Cellular and molecular immunology, Ninth edition. Elsevier.
-
- Björkström NK et al. (2016) Emerging insights into natural killer cells in human peripheral tissues. Nat. Rev. Immunol 16, 310–320 - PubMed
-
- Chiossone L et al. (2018) Natural killer cells and other innate lymphoid cells in cancer. Nat. Rev. Immunol 18, 671–688 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
