

Noninvasive Assessment of Interstitial Fibrosis and Tubular Atrophy in Renal Transplant by Combining Point-Shear Wave Elastography and Estimated Glomerular Filtration Rate
- PMID: 35054186
- PMCID: PMC8774870
- DOI: 10.3390/diagnostics12010018
Noninvasive Assessment of Interstitial Fibrosis and Tubular Atrophy in Renal Transplant by Combining Point-Shear Wave Elastography and Estimated Glomerular Filtration Rate
Abstract
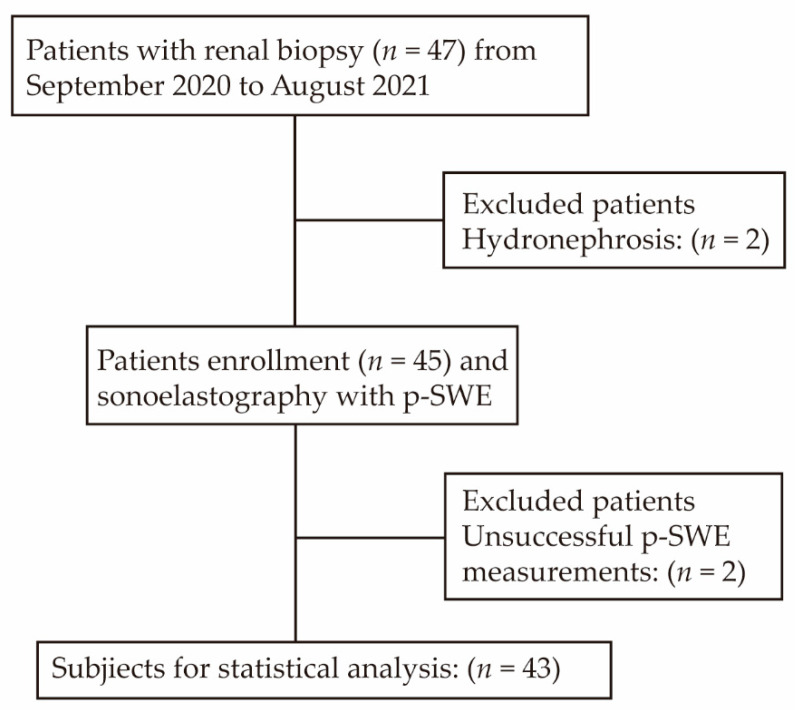
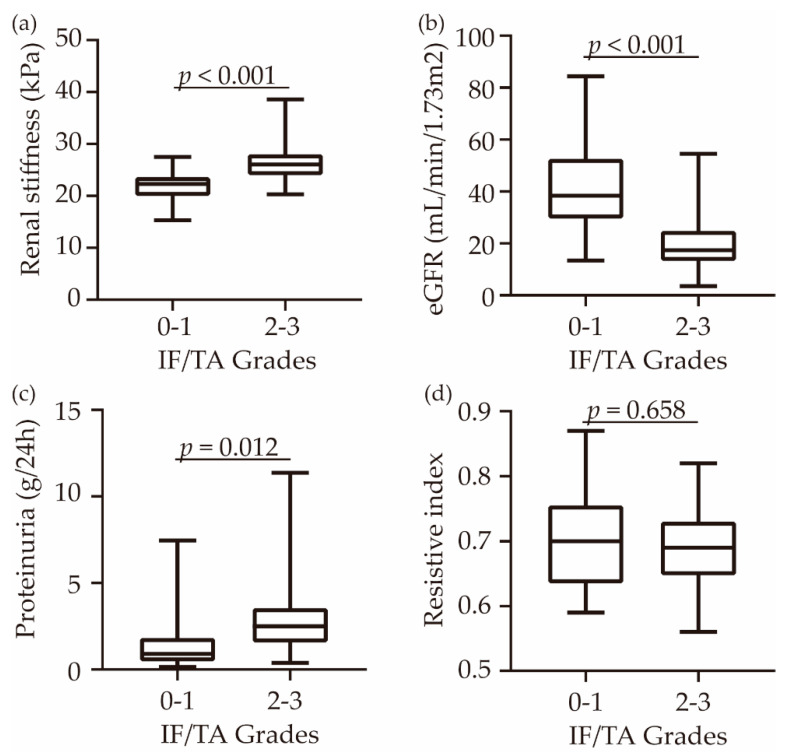
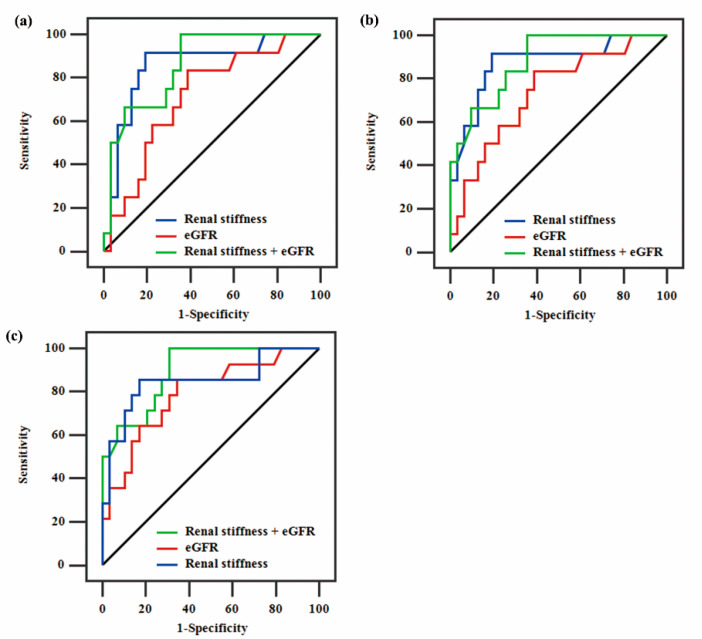
The purpose of this study was to evaluate the feasibility of the combination of point-shear wave elastography (p-SWE) and estimated glomerular filtration rate (eGFR) for assessing different stages of interstitial fibrosis and tubular atrophy (IF/TA) in patients with chronic renal allograft dysfunction (CAD). From September 2020 to August 2021, 47 patients who underwent renal biopsy and p-SWE examinations were consecutively enrolled in this study. The areas under the receiver operating characteristic curves (AUCs) were calculated to evaluate overall accuracy and to identify the optimal cutoff values for different IF/TA stages. A total of 43 patients were enrolled in this study. The renal cortical stiffness and eGFR showed a significant difference between IF/TA Grade 0-1 and Grade 2-3 (p < 0.001). Additionally, renal stiffness and eGFR were independent predictors for moderate-to-severe IF/TA (Grade ≥ 2) according to multiple logistic regression analysis. The combination of p-SWE and eGFR, with an optimal cutoff value of -1.63, was superior to eGFR alone in assessing moderate-to-severe interstitial fibrosis (AUC, 0.86 vs. 0.72, p = 0.02) or tubular atrophy (AUC, 0.88 vs. 0.74, p = 0.02). There was no difference between p-SWE and eGFR in assessing moderate-to-severe IF/TA (AUC, 0.85 vs. 0.79, p = 0.61). Therefore, combining p-SWE and eGFR is worthy of clinical popularization and application.
Keywords: estimated glomerular filtration; interstitial fibrosis and tubular atrophy; point-shear wave elastography; renal transplantation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Integrating shear wave elastography and estimated glomerular filtration rate to enhance diagnostic strategy for renal fibrosis assessment in chronic kidney disease.Quant Imaging Med Surg. 2024 Feb 1;14(2):1766-1777. doi: 10.21037/qims-23-962. Epub 2024 Jan 2. Quant Imaging Med Surg. 2024. PMID: 38415158 Free PMC article.
-
Evaluation of renal fibrosis in patients with chronic kidney disease by shear wave elastography: a comparative analysis with pathological findings.Abdom Radiol (NY). 2022 Feb;47(2):738-745. doi: 10.1007/s00261-021-03351-x. Epub 2021 Nov 20. Abdom Radiol (NY). 2022. PMID: 34800163
-
Doppler ultrasound imaging and shear wave elastography for evaluation of interstitial fibrosis/tubular atrophy in IgA nephropathy.Abdom Radiol (NY). 2024 Oct 10. doi: 10.1007/s00261-024-04613-0. Online ahead of print. Abdom Radiol (NY). 2024. PMID: 39387885
-
Role of Shear Wave Elastography for Assessment of Renal-Allograft Fibrosis and its Correlation With Histopathology.J Ultrasound Med. 2024 Oct;43(10):1979-1992. doi: 10.1002/jum.16532. Epub 2024 Jul 30. J Ultrasound Med. 2024. PMID: 39076034
-
Chronic allograft nephropathy or interstitial fibrosis and tubular atrophy: what is in a name?Curr Opin Nephrol Hypertens. 2014 May;23(3):245-50. doi: 10.1097/01.mnh.0000444811.26884.2d. Curr Opin Nephrol Hypertens. 2014. PMID: 24626060 Review.
Cited by
-
Multimodal ultrasound deep learning to detect fibrosis in early chronic kidney disease.Ren Fail. 2024 Dec;46(2):2417740. doi: 10.1080/0886022X.2024.2417740. Epub 2024 Oct 22. Ren Fail. 2024. PMID: 39435700 Free PMC article.
-
Investigating the role of ultrasound-based shear wave elastography in kidney transplanted patients: correlation between non-invasive fibrosis detection, kidney dysfunction and biopsy results-a systematic review and meta-analysis.J Nephrol. 2024 Jul;37(6):1509-1522. doi: 10.1007/s40620-023-01856-w. Epub 2024 Mar 1. J Nephrol. 2024. PMID: 38427308 Free PMC article.
-
Application of ultrasound in early prediction of delayed graft function after renal transplantation.Abdom Radiol (NY). 2024 Oct;49(10):3548-3558. doi: 10.1007/s00261-024-04353-1. Epub 2024 May 17. Abdom Radiol (NY). 2024. PMID: 38760530 Review.
-
Ultrasound elastography in chronic kidney disease: a systematic review and meta-analysis.J Med Ultrason (2001). 2023 Jul;50(3):381-415. doi: 10.1007/s10396-023-01304-z. Epub 2023 Apr 25. J Med Ultrason (2001). 2023. PMID: 37186192 Review.
References
-
- Tong A., Sautenet B., Poggio E.D., Lentine K.L., Oberbauer R., Mannon R., Murphy B., Padilla B., Chow K.M., Marson L., et al. Establishing a Core Outcome Measure for Graft Health: A Standardized Outcomes in Nephrology-Kidney Transplantation (SONG-Tx) Consensus Workshop Report. Transplantation. 2018;102:1358–1366. doi: 10.1097/TP.0000000000002125. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
