

Intestinal Barrier and Permeability in Health, Obesity and NAFLD
- PMID: 35052763
- PMCID: PMC8773010
- DOI: 10.3390/biomedicines10010083
Intestinal Barrier and Permeability in Health, Obesity and NAFLD
Abstract
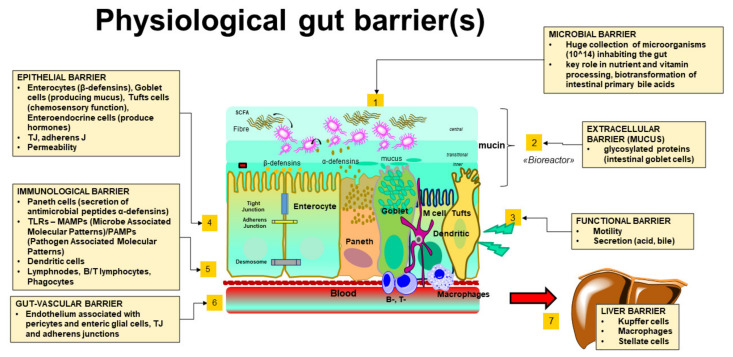
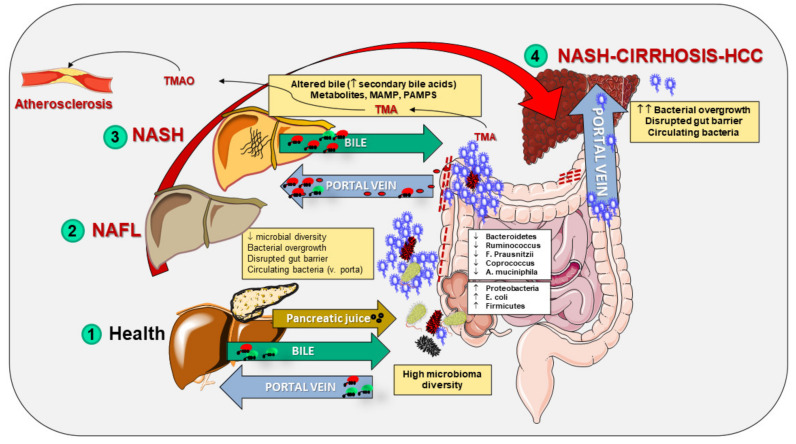
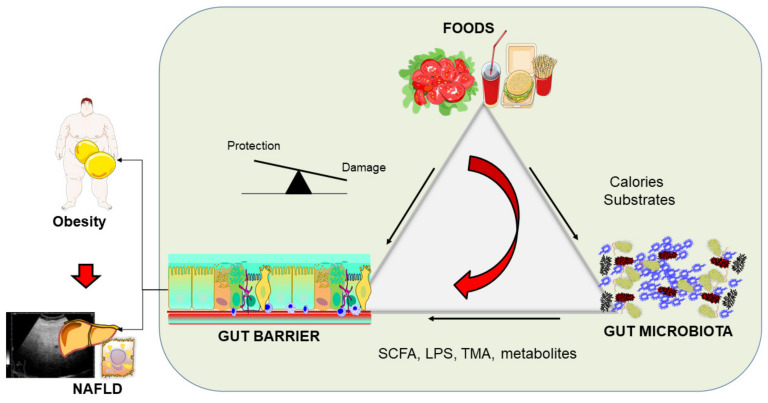
The largest surface of the human body exposed to the external environment is the gut. At this level, the intestinal barrier includes luminal microbes, the mucin layer, gastrointestinal motility and secretion, enterocytes, immune cells, gut vascular barrier, and liver barrier. A healthy intestinal barrier is characterized by the selective permeability of nutrients, metabolites, water, and bacterial products, and processes are governed by cellular, neural, immune, and hormonal factors. Disrupted gut permeability (leaky gut syndrome) can represent a predisposing or aggravating condition in obesity and the metabolically associated liver steatosis (nonalcoholic fatty liver disease, NAFLD). In what follows, we describe the morphological-functional features of the intestinal barrier, the role of major modifiers of the intestinal barrier, and discuss the recent evidence pointing to the key role of intestinal permeability in obesity/NAFLD.
Keywords: intestine; metabolic syndrome; metabolome; microbiota.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Intestinal Barrier Function in the Pathogenesis of Nonalcoholic Fatty Liver Disease.J Clin Transl Hepatol. 2023 Apr 28;11(2):452-458. doi: 10.14218/JCTH.2022.00089. Epub 2022 Aug 22. J Clin Transl Hepatol. 2023. PMID: 36643028 Free PMC article. Review.
-
Liver Steatosis, Gut-Liver Axis, Microbiome and Environmental Factors. A Never-Ending Bidirectional Cross-Talk.J Clin Med. 2020 Aug 14;9(8):2648. doi: 10.3390/jcm9082648. J Clin Med. 2020. PMID: 32823983 Free PMC article. Review.
-
The role of microbiota in nonalcoholic fatty liver disease.Eur J Clin Invest. 2022 Jul;52(7):e13768. doi: 10.1111/eci.13768. Epub 2022 Mar 26. Eur J Clin Invest. 2022. PMID: 35294774 Review.
-
Gut microbiota, intestinal permeability, and systemic inflammation: a narrative review.Intern Emerg Med. 2024 Mar;19(2):275-293. doi: 10.1007/s11739-023-03374-w. Epub 2023 Jul 28. Intern Emerg Med. 2024. PMID: 37505311 Free PMC article. Review.
-
Can You Trust Your Gut? Implicating a Disrupted Intestinal Microbiome in the Progression of NAFLD/NASH.Front Endocrinol (Lausanne). 2020 Oct 21;11:592157. doi: 10.3389/fendo.2020.592157. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33193105 Free PMC article. Review.
Cited by
-
Polyphenols improve non-alcoholic fatty liver disease via gut microbiota: A comprehensive review.Food Sci Nutr. 2024 Jun 7;12(8):5341-5356. doi: 10.1002/fsn3.4178. eCollection 2024 Aug. Food Sci Nutr. 2024. PMID: 39139973 Free PMC article. Review.
-
Intestinal Ecology Changes in Diarrheic Père David's Deer Revealed by Gut Microbiota and Fecal Metabolites Analysis.Animals (Basel). 2022 Nov 30;12(23):3366. doi: 10.3390/ani12233366. Animals (Basel). 2022. PMID: 36496887 Free PMC article.
-
Nonalcoholic fatty liver disease and diabetes.World J Diabetes. 2022 Sep 15;13(9):668-682. doi: 10.4239/wjd.v13.i9.668. World J Diabetes. 2022. PMID: 36188142 Free PMC article. Review.
-
Obesity and Its Multiple Clinical Implications between Inflammatory States and Gut Microbiotic Alterations.Diseases. 2022 Dec 29;11(1):7. doi: 10.3390/diseases11010007. Diseases. 2022. PMID: 36648872 Free PMC article. Review.
-
RNAseq of Osteoarthritic Synovial Tissues: Systematic Literary Review.Front Aging. 2022 May 25;3:836791. doi: 10.3389/fragi.2022.836791. eCollection 2022. Front Aging. 2022. PMID: 35821799 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
