

Oral Cancer Stem Cells: Therapeutic Implications and Challenges
- PMID: 35048028
- PMCID: PMC8757826
- DOI: 10.3389/froh.2021.685236
Oral Cancer Stem Cells: Therapeutic Implications and Challenges
Abstract
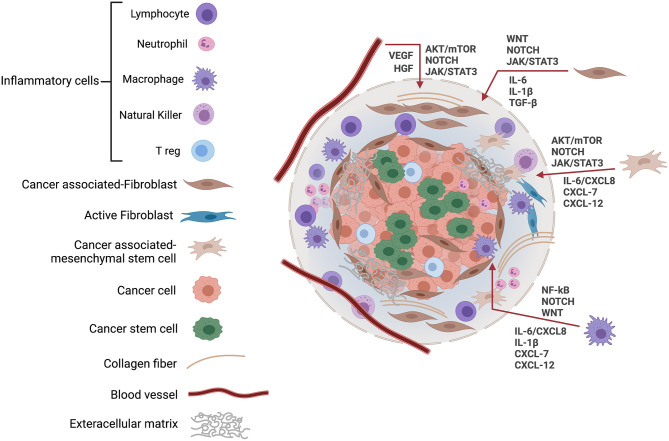
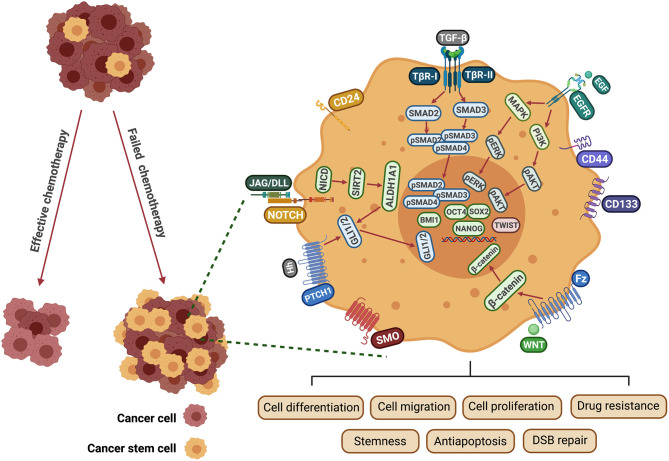
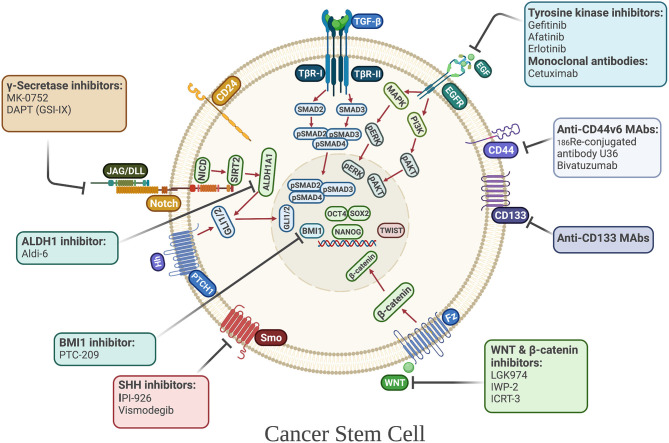
Head and neck squamous cell carcinoma (HNSCC) is currently one of the 10 most common malignancies worldwide, characterized by a biologically highly diverse group of tumors with non-specific biomarkers and poor prognosis. The incidence rate of HNSCC varies widely throughout the world, with an evident prevalence in developing countries such as those in Southeast Asia and Southern Africa. Tumor relapse and metastasis following traditional treatment remain major clinical problems in oral cancer management. Current evidence suggests that therapeutic resistance and metastasis of cancer are mainly driven by a unique subpopulation of tumor cells, termed cancer stem cells (CSCs), or cancer-initiating cells (CICs), which are characterized by their capacity for self-renewal, maintenance of stemness and increased tumorigenicity. Thus, more understanding of the molecular mechanisms of CSCs and their behavior may help in developing effective therapeutic interventions that inhibit tumor growth and progression. This review provides an overview of the main signaling cascades in CSCs that drive tumor repropagation and metastasis in oral cancer, with a focus on squamous cell carcinoma. Other oral non-SCC tumors, including melanoma and malignant salivary gland tumors, will also be considered. In addition, this review discusses some of the CSC-targeted therapeutic strategies that have been employed to combat disease progression, and the challenges of targeting CSCs, with the aim of improving the clinical outcomes for patients with oral malignancies. Targeting of CSCs in head and neck cancer (HNC) represents a promising approach to improve disease outcome. Some CSC-targeted therapies have already been proven to be successful in pre-clinical studies and they are now being tested in clinical trials, mainly in combination with conventional treatment regimens. However, some studies revealed that CSCs may not be the only players that control disease relapse and progression of HNC. Further, clinical research studying a combination of therapies targeted against head and neck CSCs may provide significant advances.
Keywords: cancer stem cells; head and neck; self-renewal; squamous cell carcinoma; targeted therapy; tumor relapse.
Copyright © 2021 Shahoumi.
Conflict of interest statement
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Cancer Stem Cells in Oral Squamous Cell Carcinoma: A Narrative Review on Experimental Characteristics and Methodological Challenges.Biomedicines. 2024 Sep 16;12(9):2111. doi: 10.3390/biomedicines12092111. Biomedicines. 2024. PMID: 39335624 Free PMC article. Review.
-
Cancer Stem Cells in Head and Neck Carcinomas: Identification and Possible Therapeutic Implications.Adv Exp Med Biol. 2018;1083:89-102. doi: 10.1007/5584_2017_116. Adv Exp Med Biol. 2018. PMID: 29139089 Review.
-
Cancer stem cells enrichment with surface markers CD271 and CD44 in human head and neck squamous cell carcinomas.Carcinogenesis. 2020 Jun 17;41(4):458-466. doi: 10.1093/carcin/bgz182. Carcinogenesis. 2020. PMID: 31742606 Free PMC article.
-
Emergence of cancer stem cells in head and neck squamous cell carcinoma: A therapeutic insight with literature review.Dent Res J (Isfahan). 2012 May;9(3):239-44. Dent Res J (Isfahan). 2012. Retraction in: Dent Res J (Isfahan). 2015 Sep-Oct;12(5):498. doi: 10.4103/1735-3327.166239. PMID: 23087725 Free PMC article. Retracted.
-
Mechanisms involved in cancer stem cell resistance in head and neck squamous cell carcinoma.Cancer Drug Resist. 2023 Feb 21;6(1):116-137. doi: 10.20517/cdr.2022.107. eCollection 2023. Cancer Drug Resist. 2023. PMID: 37065869 Free PMC article. Review.
Cited by
-
Umbrella Review on Cancer Stem Cell in Oral and Head and Neck Squamous Cell Carcinoma.J Stem Cells Regen Med. 2023 Dec 31;19(2):29-33. doi: 10.46582/jsrm.1902007. eCollection 2023. J Stem Cells Regen Med. 2023. PMID: 38406617 Free PMC article. Review.
-
Mechanisms of Melanoma Progression and Treatment Resistance: Role of Cancer Stem-like Cells.Cancers (Basel). 2024 Jan 22;16(2):470. doi: 10.3390/cancers16020470. Cancers (Basel). 2024. PMID: 38275910 Free PMC article. Review.
-
Cancer Stem Cells in Oral Squamous Cell Carcinoma: A Narrative Review on Experimental Characteristics and Methodological Challenges.Biomedicines. 2024 Sep 16;12(9):2111. doi: 10.3390/biomedicines12092111. Biomedicines. 2024. PMID: 39335624 Free PMC article. Review.
-
The Role of Hedgehog Signaling Pathway in Head and Neck Squamous Cell Carcinoma.Cells. 2023 Aug 17;12(16):2083. doi: 10.3390/cells12162083. Cells. 2023. PMID: 37626893 Free PMC article. Review.
-
Diversity of the Origin of Cancer Stem Cells in Oral Squamous Cell Carcinoma and Its Clinical Implications.Cancers (Basel). 2022 Jul 22;14(15):3588. doi: 10.3390/cancers14153588. Cancers (Basel). 2022. PMID: 35892847 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials