

Comparison of the Accuracy and Completeness of Records of Serious Vascular Events in Routinely Collected Data vs Clinical Trial-Adjudicated Direct Follow-up Data in the UK: Secondary Analysis of the ASCEND Randomized Clinical Trial
- PMID: 34962561
- PMCID: PMC8715347
- DOI: 10.1001/jamanetworkopen.2021.39748
Comparison of the Accuracy and Completeness of Records of Serious Vascular Events in Routinely Collected Data vs Clinical Trial-Adjudicated Direct Follow-up Data in the UK: Secondary Analysis of the ASCEND Randomized Clinical Trial
Abstract
Importance: Routinely collected data could substantially decrease the cost of conducting trials.
Objective: To assess the accuracy and completeness of UK routine data for ascertaining serious vascular events (SVEs) compared with adjudicated follow-up data.
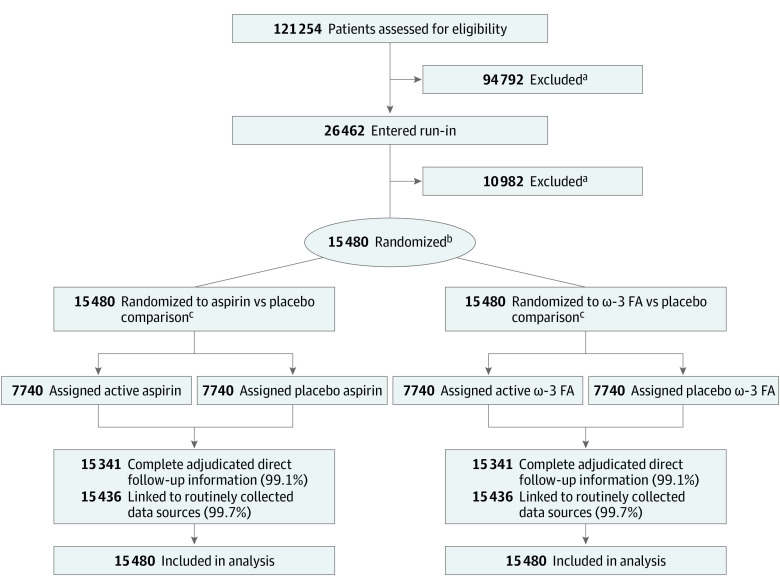
Design, setting, and participants: This was a secondary analysis of a randomized clinical trial. From June 24, 2005, to July 28, 2011, the ASCEND (A Study of Cardiovascular Events in Diabetes) primary prevention trial used mail-based methods to randomize people with diabetes without evidence of atherosclerotic vascular disease using a 2 × 2 factorial design to aspirin and/or ω-fatty acids vs matching placebo in the UK. Direct participant mail-based follow-up was the main source of outcome data, with more than 90% of the primary outcome events undergoing adjudication. Follow-up was completed on July 31, 2017. In parallel, more than 99% of participants were linked to routinely collected hospital admission and death registry data (ie, routine data), enabling post hoc randomized comparisons of different sources of outcome data (conducted from September 1, 2018, to October 1, 2021).
Interventions: Random allocation to 100 mg of aspirin once daily vs matching placebo and separately to 1 g of ω-3 fatty acids once daily vs placebo.
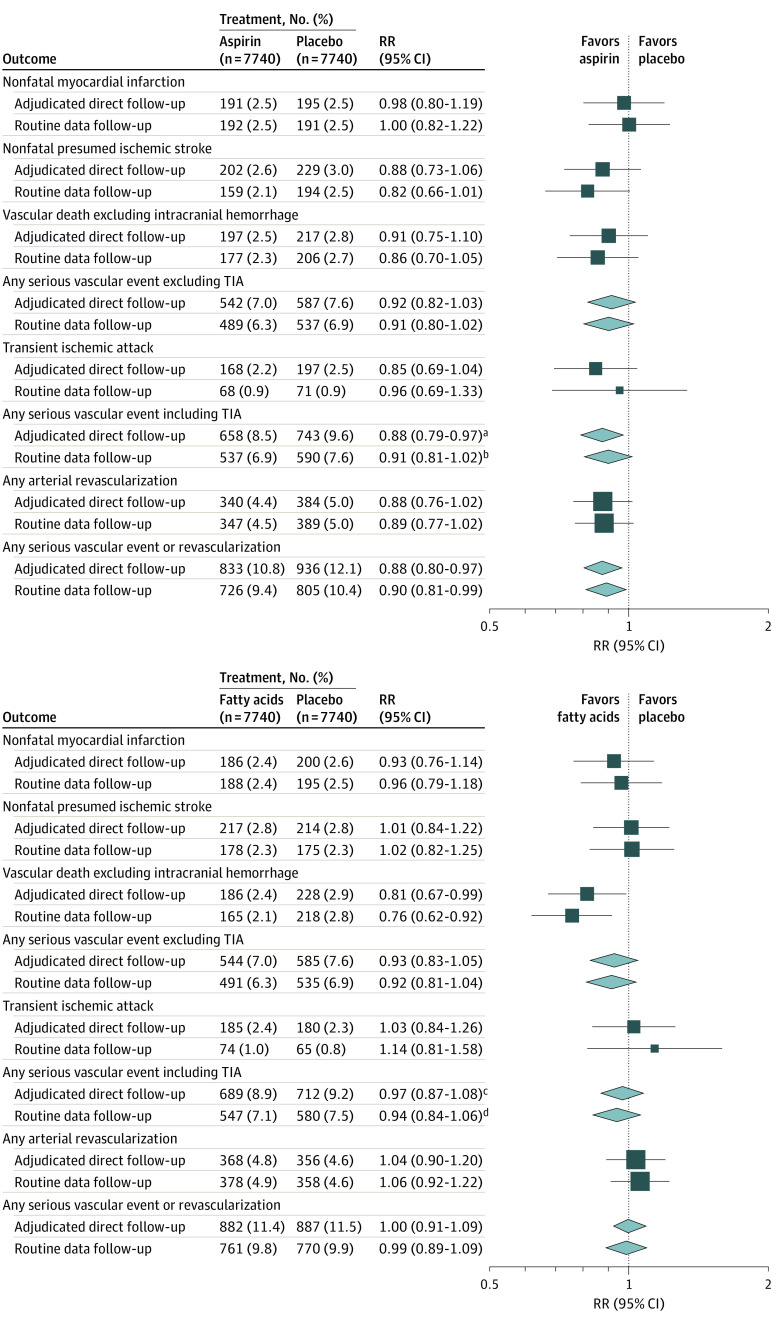
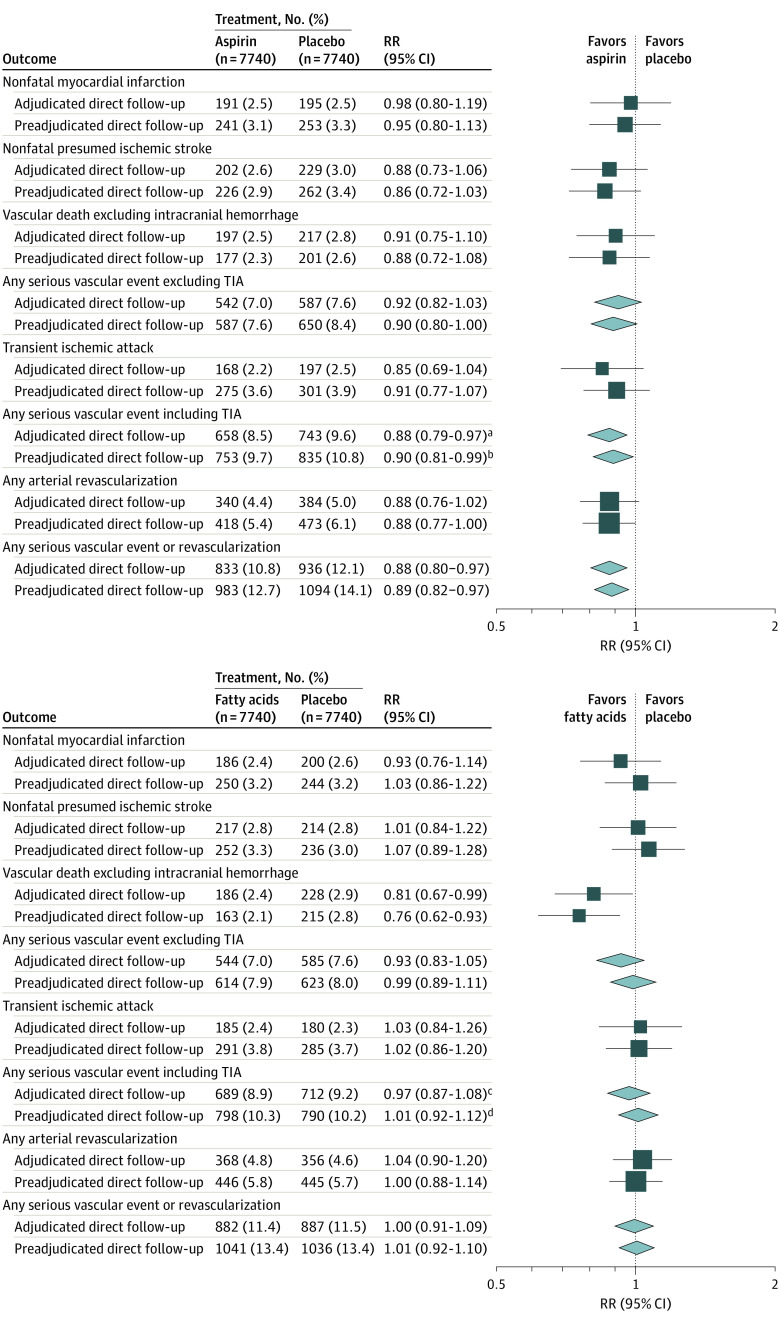
Main outcomes and measures: The primary outcome consisted of SVEs (a composite of nonfatal myocardial infarction, ischemic stroke, transient ischemic attack [TIA], or vascular death, excluding hemorrhagic stroke).
Results: A total of 15 480 participants were randomized (mean [SD] age, 63 [9] years; 9684 [62.6%] men) and followed up for a mean (SD) of 7.4 (1.8) years. For SVEs, agreement between adjudicated direct follow-up and routine data sources was strong (1401 vs 1127 events; κ = 0.78 [95% CI, 0.76-0.80]; sensitivity, 72.0% [95% CI, 69.7%-74.4%]; specificity, 99.2% [95% CI, 99.0%-99.3%]), and sensitivity improved for SVEs excluding transient ischemic attack (1129 vs 1026 events; sensitivity, 80.6% [95% CI, 78.3%-82.9%]). Rate ratios for the aspirin-randomized comparison for adjudicated direct follow-up vs follow-up solely through routine data alone were 0.88 (95% CI, 0.79-0.97) vs 0.91 (95% CI, 0.81-1.02) for the primary outcome and 0.92 (95% CI, 0.82-1.03) vs 0.91 (95% CI, 0.80-1.02) for SVEs excluding TIA. Results were similar for the ω-3 fatty acid comparison, and adjudication did not seem to markedly change rate ratios.
Conclusions and relevance: Post hoc analyses of the ASCEND trial suggest that routinely collected hospital admission and death registry data in the UK could be used as the sole method of follow-up for myocardial infarction, ischemic stroke resulting in hospitalization, vascular death, and arterial revascularization in primary prevention cardiovascular trials, without the need for verification by clinical adjudication.
Conflict of interest statement
Figures
Comment in
-
Pragmatic Clinical Trials-Ready for Prime Time?JAMA Netw Open. 2021 Dec 1;4(12):e2140212. doi: 10.1001/jamanetworkopen.2021.40212. JAMA Netw Open. 2021. PMID: 34962564 No abstract available.
Similar articles
-
Low-dose aspirin for primary prevention of cardiovascular events in Japanese patients 60 years or older with atherosclerotic risk factors: a randomized clinical trial.JAMA. 2014 Dec 17;312(23):2510-20. doi: 10.1001/jama.2014.15690. JAMA. 2014. PMID: 25401325 Clinical Trial.
-
Assessment of the End Point Adjudication Process on the Results of the Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke (POINT) Trial: A Secondary Analysis.JAMA Netw Open. 2019 Sep 4;2(9):e1910769. doi: 10.1001/jamanetworkopen.2019.10769. JAMA Netw Open. 2019. PMID: 31490536 Free PMC article.
-
Comparison of Investigator-Reported vs Centrally Adjudicated Major Adverse Cardiac Events: A Secondary Analysis of the COMPASS Trial.JAMA Netw Open. 2022 Nov 1;5(11):e2243201. doi: 10.1001/jamanetworkopen.2022.43201. JAMA Netw Open. 2022. PMID: 36409491 Free PMC article. Clinical Trial.
-
Dipyridamole for preventing stroke and other vascular events in patients with vascular disease.Cochrane Database Syst Rev. 2003;(1):CD001820. doi: 10.1002/14651858.CD001820. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2006 Apr 19;(2):CD001820. doi: 10.1002/14651858.CD001820.pub2 PMID: 12535415 Updated. Review.
-
Clopidogrel and modified-release dipyridamole for the prevention of occlusive vascular events (review of Technology Appraisal No. 90): a systematic review and economic analysis.Health Technol Assess. 2011 Sep;15(31):1-178. doi: 10.3310/hta15310. Health Technol Assess. 2011. PMID: 21888837 Free PMC article. Review.
Cited by
-
Concordance between clinical outcomes in the Systolic Blood Pressure Intervention Trial and in the electronic health record.Contemp Clin Trials. 2023 May;128:107172. doi: 10.1016/j.cct.2023.107172. Epub 2023 Mar 31. Contemp Clin Trials. 2023. PMID: 37004812 Free PMC article. Clinical Trial.
-
Reliability of major bleeding events in UK routine data versus clinical trial adjudicated follow-up data.Heart. 2023 Sep 13;109(19):1467-1472. doi: 10.1136/heartjnl-2023-322616. Heart. 2023. PMID: 37270201 Free PMC article. Clinical Trial.
-
Feasibility of randomizing Danish citizens aged 65-79 years to high-dose quadrivalent influenza vaccine vs. standard-dose quadrivalent influenza vaccine in a pragmatic registry-based setting: rationale and design of the DANFLU-1 Trial.Pilot Feasibility Stud. 2022 Apr 21;8(1):87. doi: 10.1186/s40814-022-01044-w. Pilot Feasibility Stud. 2022. PMID: 35449028 Free PMC article.
-
Randomised controlled trial of population screening for atrial fibrillation in people aged 70 years and over to reduce stroke: protocol for the SAFER trial.BMJ Open. 2024 Apr 25;14(4):e082047. doi: 10.1136/bmjopen-2023-082047. BMJ Open. 2024. PMID: 38670614 Free PMC article.
-
Unstable Angina as a Component of Primary Composite Endpoints in Clinical Cardiovascular Trials: Pros and Cons.Cardiology. 2022;147(3):235-247. doi: 10.1159/000524948. Epub 2022 May 10. Cardiology. 2022. PMID: 35537418 Free PMC article. Review.
References
-
- European Society of Cardiology . Clinical practice guidelines. Accessed February 17, 2021. https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines
-
- Collins R. Back to the future: the urgent need to re-introduce streamlined trials. Eur Heart J Suppl. 2018;20(suppl C):C14-C17. doi:10.1093/eurheartj/suy001 - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
