

A Visual and Comprehensive Review on COVID-19-Associated Pulmonary Aspergillosis (CAPA)
- PMID: 34947049
- PMCID: PMC8708864
- DOI: 10.3390/jof7121067
A Visual and Comprehensive Review on COVID-19-Associated Pulmonary Aspergillosis (CAPA)
Abstract
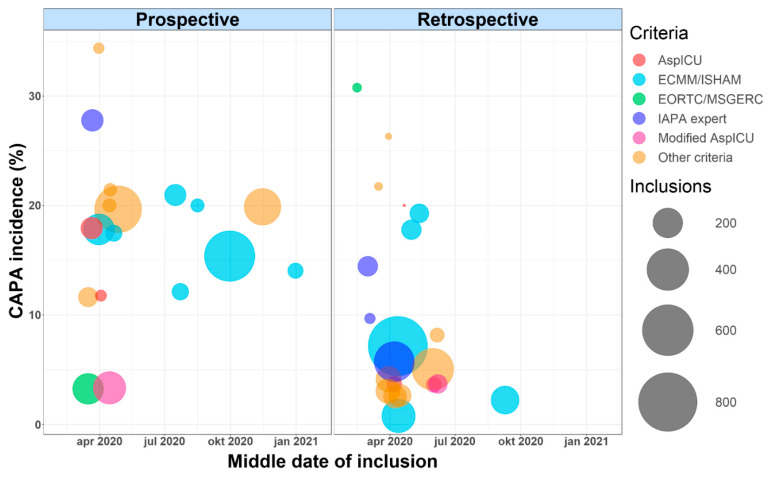
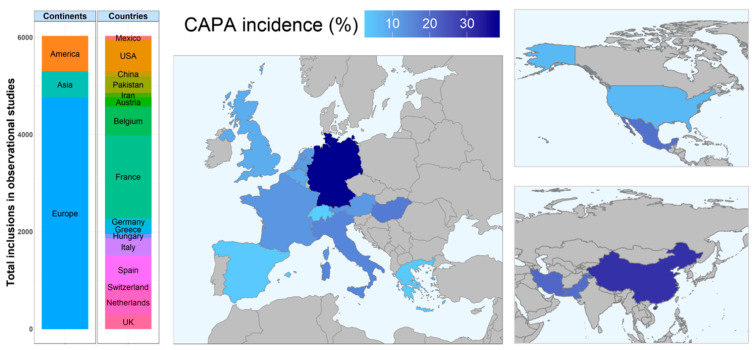
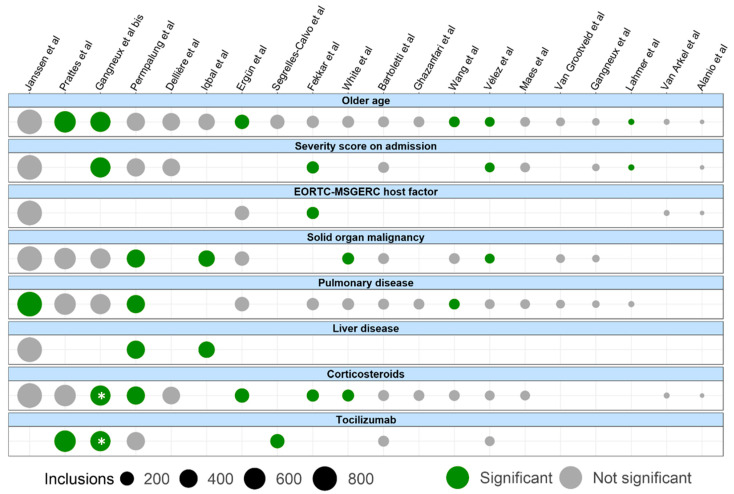
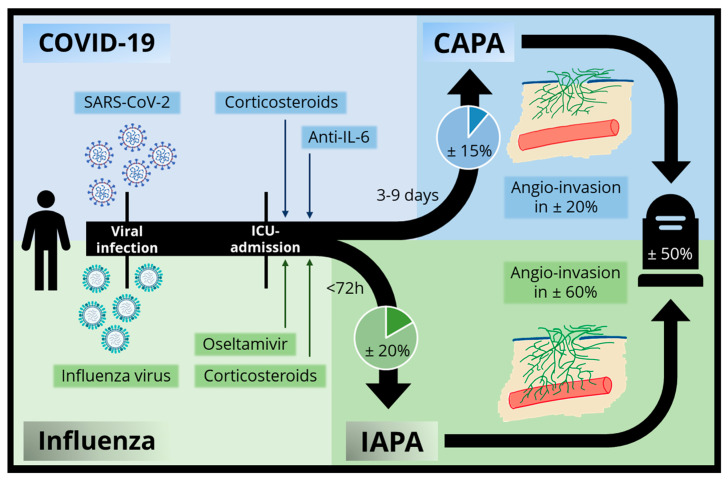
Coronavirus disease 19 (COVID-19)-associated pulmonary aspergillosis (CAPA) is a severe fungal infection complicating critically ill COVID-19 patients. Numerous retrospective and prospective studies have been performed to get a better grasp on this lethal co-infection. We performed a qualitative review and summarized data from 48 studies in which 7047 patients had been included, of whom 820 had CAPA. The pooled incidence of proven, probable or putative CAPA was 15.1% among 2953 ICU-admitted COVID-19 patients included in 18 prospective studies. Incidences showed great variability due to multiple factors such as discrepancies in the rate and depth of the fungal work-up. The pathophysiology and risk factors for CAPA are ill-defined, but therapy with corticosteroids and anti-interleukin-6 therapy potentially confer the biggest risk. Sampling for mycological work-up using bronchoscopy is the cornerstone for diagnosis, as imaging is often aspecific. CAPA is associated with an increased mortality, but we do not have conclusive data whether therapy contributes to an increased survival in these patients. We conclude our review with a comparison between influenza-associated pulmonary aspergillosis (IAPA) and CAPA.
Keywords: COVID-19; COVID-19-associated pulmonary aspergillosis (CAPA); IAPA; aspergillosis; critical care; influenza; influenza-associated pulmonary aspergillosis; intensive care unit.
Conflict of interest statement
S.F. is funded by a Research Foundation Flanders (FWO) PhD fellowship (11M6922N) and declares travel support from Pfizer. K.L. received consultancy fees from MRM Health, MSD and Gilead, speaker fees from FUJIFILM WAKO, Pfizer and Gilead and a service fee from Thermo Fisher Scientific. I.S. is supported by the Clinical Research Fund of UZ Leuven and served as a consultant to and has received unrestricted travel and research grants from Gilead Sciences, Merck Sharpe and Dohme Corp., Pfizer, Inc. and Cidara. G.D. declares advisory board participation (Pfizer, Gilead) and lecture fees from Gilead and Pfizer. J.W. has received investigator-initiated grants from Pfizer, Gilead and MSD and speakers’ and travel fees from Pfizer, Gilead and MSD. The other authors report no conflict of interest.
Figures
Similar articles
-
Lung epithelial and myeloid innate immunity in influenza-associated or COVID-19-associated pulmonary aspergillosis: an observational study.Lancet Respir Med. 2022 Dec;10(12):1147-1159. doi: 10.1016/S2213-2600(22)00259-4. Epub 2022 Aug 24. Lancet Respir Med. 2022. PMID: 36029799 Free PMC article.
-
Risk factors and the value of microbiological examinations of COVID-19 associated pulmonary aspergillosis in critically ill patients in intensive care unit: the appropriate microbiological examinations are crucial for the timely diagnosis of CAPA.Front Cell Infect Microbiol. 2023 Nov 21;13:1287496. doi: 10.3389/fcimb.2023.1287496. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 38076456 Free PMC article.
-
COVID-19-Associated Pulmonary Aspergillosis (CAPA).J Intensive Med. 2021 Aug 7;1(2):71-80. doi: 10.1016/j.jointm.2021.07.001. eCollection 2021 Oct. J Intensive Med. 2021. PMID: 36785564 Free PMC article. Review.
-
Influenza- and COVID-19-Associated Pulmonary Aspergillosis: Are the Pictures Different?J Fungi (Basel). 2021 May 15;7(5):388. doi: 10.3390/jof7050388. J Fungi (Basel). 2021. PMID: 34063556 Free PMC article.
-
Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion.Intensive Care Med. 2020 Aug;46(8):1524-1535. doi: 10.1007/s00134-020-06091-6. Epub 2020 Jun 22. Intensive Care Med. 2020. PMID: 32572532 Free PMC article.
Cited by
-
Challenges in Diagnosing COVID-19-Associated Pulmonary Aspergillosis in Critically Ill Patients: The Relationship between Case Definitions and Autoptic Data.J Fungi (Basel). 2022 Aug 23;8(9):894. doi: 10.3390/jof8090894. J Fungi (Basel). 2022. PMID: 36135619 Free PMC article.
-
Severe Recurrent COVID-Associated Pulmonary Aspergillosis: A Challenging Case.Healthcare (Basel). 2022 Dec 8;10(12):2483. doi: 10.3390/healthcare10122483. Healthcare (Basel). 2022. PMID: 36554008 Free PMC article.
-
Nebulized Amphotericin B in Mechanically Ventilated COVID-19 Patients to Prevent Invasive Pulmonary Aspergillosis: A Retrospective Cohort Study.Crit Care Explor. 2022 May 9;4(5):e0696. doi: 10.1097/CCE.0000000000000696. eCollection 2022 May. Crit Care Explor. 2022. PMID: 35558738 Free PMC article.
-
Isavuconazole for COVID-19-Associated Invasive Mold Infections.J Fungi (Basel). 2022 Jun 28;8(7):674. doi: 10.3390/jof8070674. J Fungi (Basel). 2022. PMID: 35887431 Free PMC article. Review.
-
Highlights from the Respiratory Failure and Mechanical Ventilation Conference 2024.Breathe (Sheff). 2024 Nov 12;20(3):240105. doi: 10.1183/20734735.0105-2024. eCollection 2024 Oct. Breathe (Sheff). 2024. PMID: 39534488 Free PMC article.
References
-
- Schauwvlieghe A.F.A.D., Rijnders B.J.A., Philips N., Verwijs R., Vanderbeke L., Van Tienen C., Lagrou K., Verweij P.E., Van de Veerdonk F.L., Gommers D., et al. Invasive Aspergillosis in Patients Admitted to the Intensive Care Unit with Severe Influenza: A Retrospective Cohort Study. Lancet Respir. Med. 2018;6:782–792. doi: 10.1016/S2213-2600(18)30274-1. - DOI - PubMed
-
- Donnelly J.P., Chen S.C., Kauffman C.A., Steinbach W.J., Baddley J.W., Verweij P.E., Clancy C.J., Wingard J.R., Lockhart S.R., Groll A.H., et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020;71:1367–1376. doi: 10.1093/cid/ciz1008. - DOI - PMC - PubMed
-
- Blot S.I., Taccone F.S., Van Den Abeele A.M., Bulpa P., Meersseman W., Brusselaers N., Dimopoulos G., Paiva J.A., Misset B., Rello J., et al. A Clinical Algorithm to Diagnose Invasive Pulmonary Aspergillosis in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2012;186:56–64. doi: 10.1164/rccm.201111-1978OC. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
