

Improving Immunotherapy Efficacy in Soft-Tissue Sarcomas: A Biomarker Driven and Histotype Tailored Review
- PMID: 34925348
- PMCID: PMC8678134
- DOI: 10.3389/fimmu.2021.775761
Improving Immunotherapy Efficacy in Soft-Tissue Sarcomas: A Biomarker Driven and Histotype Tailored Review
Abstract
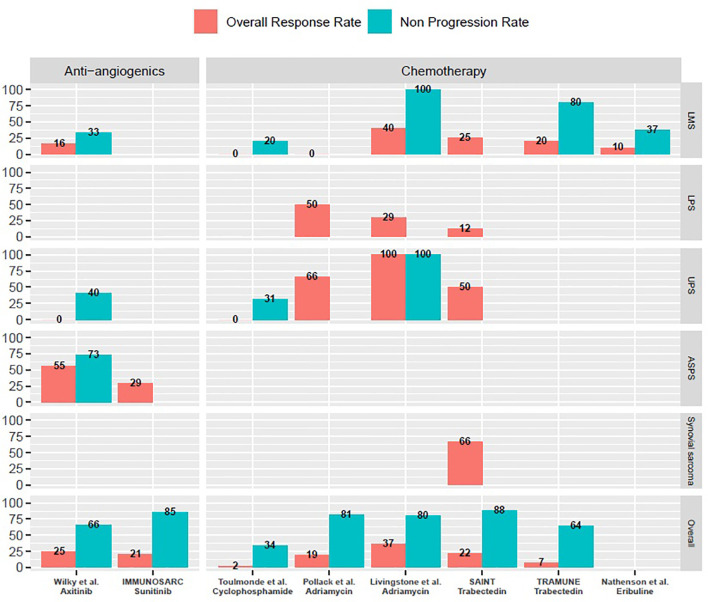
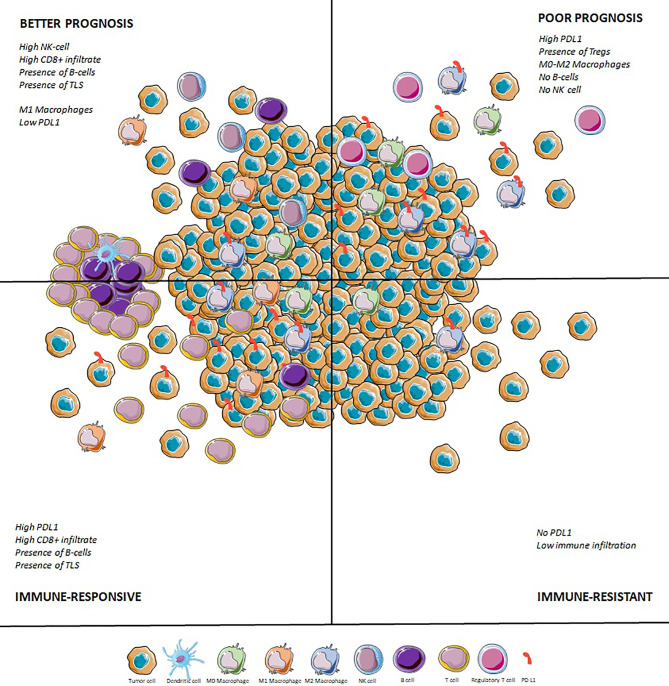
Anti-PD-(L)1 therapies yield a disappointing response rate of 15% across soft-tissue sarcomas, even if some subtypes benefit more than others. The proportions of TAMs and TILs in their tumor microenvironment are variable, and this heterogeneity correlates to histotype. Tumors with a richer CD8+ T cell, M1 macrophage, and CD20+ cells infiltrate have a better prognosis than those infiltrated by M0/M2 macrophages and a high immune checkpoint protein expression. PD-L1 and CD8+ infiltrate seem correlated to response to immune checkpoint inhibitors (ICI), but tertiary lymphoid structures have the best predictive value and have been validated prospectively. Trials for combination therapies are ongoing and focus on the association of ICI with chemotherapy, achieving encouraging results especially with pembrolizumab and doxorubicin at an early stage, or ICI with antiangiogenics. A synergy with oncolytic viruses is seen and intratumoral talimogene laherpavec yields an impressive 35% ORR when associated to pembrolizumab. Adoptive cellular therapies are also of great interest in tumors with a high expression of cancer-testis antigens (CTA), such as synovial sarcomas or myxoid round cell liposarcomas with an ORR ranging from 20 to 50%. It seems crucial to adapt the design of clinical trials to histology. Leiomyosarcomas are characterized by complex genomics but are poorly infiltrated by immune cells and do not benefit from ICI. They should be tested with PIK3CA/AKT inhibition, IDO blockade, or treatments aiming at increasing antigenicity (radiotherapy, PARP inhibitors). DDLPS are more infiltrated and have higher PD-L1 expression, but responses to ICI remain variable across clinical studies. Combinations with MDM2 antagonists or CDK4/6 inhibitors may improve responses for DDLPS. UPS harbor the highest copy number alterations (CNA) and mutation rates, with a rich immune infiltrate containing TLS. They have a promising 15-40% ORR to ICI. Trials for ICB should focus on immune-high UPS. Association of ICI with FGFR inhibitors warrants further exploration in the immune-low group of UPS. Finally translocation-related sarcomas are heterogeneous, and although synovial sarcomas a poorly infiltrated and have a poor response rate to ICI, ASPS largely benefit from ICB monotherapy or its association with antiangiogenics agents. Targeting specific neoantigens through vaccine or adoptive cellular therapies is probably the most promising approach in synovial sarcomas.
Keywords: PD1 and PDL1; combination (combined) therapy; immunotherapy; soft tissue sarcoma (STS); tertiary lymphoid structure (TLS).
Copyright © 2021 Roulleaux Dugage, Nassif, Italiano and Bahleda.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Beyond the Driver Mutation: Immunotherapies in Gastrointestinal Stromal Tumors.Front Immunol. 2021 Aug 20;12:715727. doi: 10.3389/fimmu.2021.715727. eCollection 2021. Front Immunol. 2021. PMID: 34489967 Free PMC article. Review.
-
Immunotherapy in Sarcoma: Current Data and Promising Strategies.Am Soc Clin Oncol Educ Book. 2024 Jun;44(3):e432234. doi: 10.1200/EDBK_432234. Am Soc Clin Oncol Educ Book. 2024. PMID: 38781557 Review.
-
Preferential Expression of Programmed Death Ligand 1 Protein in Tumor-Associated Macrophages and Its Potential Role in Immunotherapy for Hepatocellular Carcinoma.Int J Mol Sci. 2021 Apr 29;22(9):4710. doi: 10.3390/ijms22094710. Int J Mol Sci. 2021. PMID: 33946835 Free PMC article.
-
Tumor DNA methylation profiles correlate with response to anti-PD-1 immune checkpoint inhibitor monotherapy in sarcoma patients.J Immunother Cancer. 2021 Mar;9(3):e001458. doi: 10.1136/jitc-2020-001458. J Immunother Cancer. 2021. PMID: 33762319 Free PMC article.
-
Immunotherapy in Sarcoma: Where Do Things Stand?Surg Oncol Clin N Am. 2022 Jul;31(3):381-397. doi: 10.1016/j.soc.2022.03.004. Surg Oncol Clin N Am. 2022. PMID: 35715140 Review.
Cited by
-
Outcomes and Follow-Up Trends in Adrenal Leiomyosarcoma: A Comprehensive Literature Review and Case Report.J Clin Med. 2024 Jun 14;13(12):3499. doi: 10.3390/jcm13123499. J Clin Med. 2024. PMID: 38930027 Free PMC article. Review.
-
Treatment approaches and outcomes of major chest wall resections and reconstructions in patients with soft tissue and bone sarcomas: a retrospective observational study.J Thorac Dis. 2024 Oct 31;16(10):6863-6878. doi: 10.21037/jtd-24-472. Epub 2024 Oct 30. J Thorac Dis. 2024. PMID: 39552892 Free PMC article.
-
Comparative effects of free doxorubicin, liposome encapsulated doxorubicin and liposome co-encapsulated alendronate and doxorubicin (PLAD) on the tumor immunologic milieu in a mouse fibrosarcoma model.Nanotheranostics. 2022 Sep 1;6(4):451-464. doi: 10.7150/ntno.75045. eCollection 2022. Nanotheranostics. 2022. PMID: 36105861 Free PMC article.
-
Cuproptosis-associated lncRNAs discern prognosis and immune microenvironment in sarcoma victims.Front Cell Dev Biol. 2022 Dec 16;10:989882. doi: 10.3389/fcell.2022.989882. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 36589745 Free PMC article.
-
Identification of prognostic models for glycosylation-related subtypes and tumor microenvironment infiltration characteristics in clear cell renal cell cancer.Heliyon. 2024 Mar 13;10(6):e27710. doi: 10.1016/j.heliyon.2024.e27710. eCollection 2024 Mar 30. Heliyon. 2024. PMID: 38515689 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous