

Impact of KRAS, BRAF and microsatellite instability status after cytoreductive surgery and HIPEC in a national cohort of colorectal peritoneal metastasis patients
- PMID: 34887523
- PMCID: PMC8888568
- DOI: 10.1038/s41416-021-01620-6
Impact of KRAS, BRAF and microsatellite instability status after cytoreductive surgery and HIPEC in a national cohort of colorectal peritoneal metastasis patients
Abstract
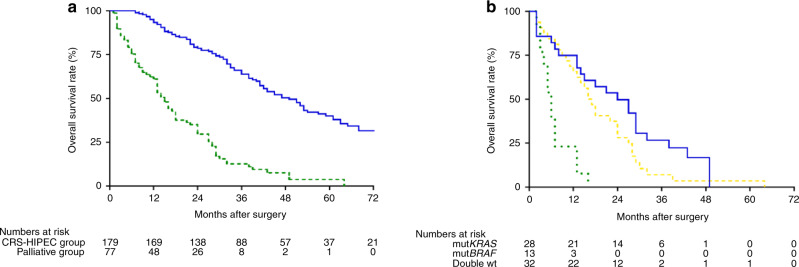
Background: Patients with metastatic colorectal cancer (mCRC) carrying BRAF (mutBRAF) or KRAS mutation (mutKRAS) have an inferior prognosis after liver or lung surgery, whereas the prognostic role in the context of peritoneal metastasis (PM) after cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) has been less investigated.
Methods: In total, 257 patients with non-appendiceal PM-CRC were included from the Norwegian National Unit for CRS-HIPEC.
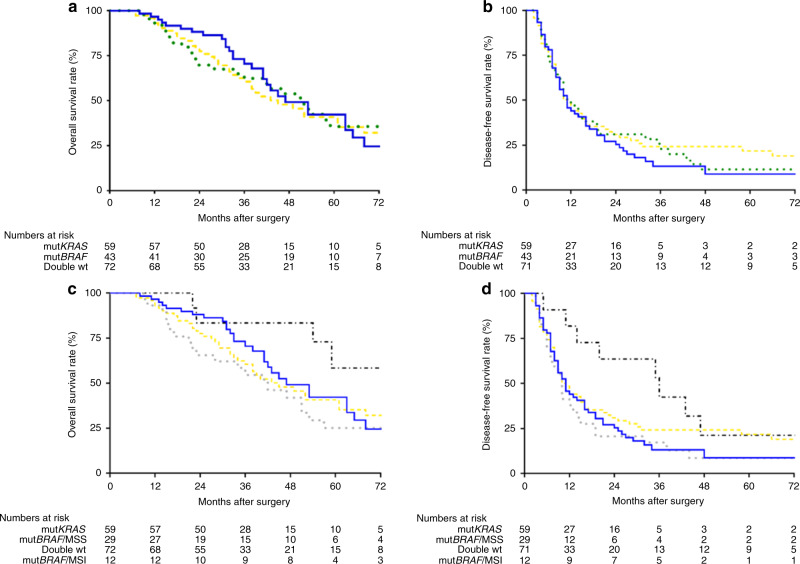
Results: In total, 180 patients received CRS-HIPEC with Mitomycin C, 77 patients received palliative surgery only. In the CRS-HIPEC group, mutBRAF was found in 24.7%, mutKRAS 33.9% and double wild-type 41.4% without differences in survival. MSI was found in 29.3% of mutBRAF cases. Patients with mutBRAF/MSI had superior 5-year survival compared to mutBRAF with MSS (58.3% vs 25.2%, P = 0.022), and better 3-year disease-free survival (DFS) compared to mutKRAS (48.6% vs 17.2%, P = 0.049). Peritoneal Cancer Index and the number of lymph node metastasis were prognostic for OS, and the same two, location and gender prognostic for DFS in multivariate analysis.
Conclusions: PM-CRC with CRS-HIPEC patients has a surprisingly high proportion of mutBRAF (24.7%). Survival was similar comparing mutBRAF, mutKRAS and double wild-type cases, whereas a small subgroup with mutBRAF and MSI had better survival. Patients with mutBRAF tumours and limited PM should be considered for CRS-HIPEC.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Microsatellite and RAS/RAF Mutational Status as Prognostic Factors in Colorectal Peritoneal Metastases Treated with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC).Ann Surg Oncol. 2022 Jun;29(6):3405-3417. doi: 10.1245/s10434-021-11045-3. Epub 2021 Nov 16. Ann Surg Oncol. 2022. PMID: 34783946
-
Effect of RAS and BRAF mutations on peritoneal metastasis risk and cytoreductive surgery/hyperthermic intraperitoneal chemotherapy efficacy in colorectal cancer: A systematic review and meta-analysis.Eur J Surg Oncol. 2024 Sep;50(9):108474. doi: 10.1016/j.ejso.2024.108474. Epub 2024 Jun 5. Eur J Surg Oncol. 2024. PMID: 38870874
-
Microsatellite instability should not determine candidacy for cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion in patients with peritoneal metastases from colorectal cancer.J Gastrointest Surg. 2024 Sep;28(9):1493-1497. doi: 10.1016/j.gassur.2024.06.019. Epub 2024 Jun 24. J Gastrointest Surg. 2024. PMID: 38925340
-
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) for colorectal and appendiceal peritoneal metastases - The Hong Kong experience and literature review.Asian J Surg. 2021 Jan;44(1):221-228. doi: 10.1016/j.asjsur.2020.05.010. Epub 2020 Jun 27. Asian J Surg. 2021. PMID: 32605790 Review.
-
Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy in the Management of Colorectal Peritoneal Metastasis.Surg Clin North Am. 2017 Jun;97(3):671-682. doi: 10.1016/j.suc.2017.01.013. Surg Clin North Am. 2017. PMID: 28501254 Review.
Cited by
-
Novel drug resistance mechanisms and drug targets in BRAF-mutated peritoneal metastasis from colorectal cancer.J Transl Med. 2024 Jul 9;22(1):646. doi: 10.1186/s12967-024-05467-2. J Transl Med. 2024. PMID: 38982444 Free PMC article.
-
Survival of Patients with Deficient Mismatch Repair Versus Proficient Mismatch Repair Metastatic Colorectal Cancer Receiving Curative-Intent Local Treatment of Metastases in a Nationwide Cohort.Ann Surg Oncol. 2023 Oct;30(11):6762-6770. doi: 10.1245/s10434-023-13974-7. Epub 2023 Aug 1. Ann Surg Oncol. 2023. PMID: 37528303 Free PMC article.
-
Impact of Molecular Status on Cytoreductive Surgery for Peritoneal Metastases from Colorectal Cancer.Clin Colon Rectal Surg. 2023 Apr 16;36(6):415-422. doi: 10.1055/s-0043-1767705. eCollection 2023 Nov. Clin Colon Rectal Surg. 2023. PMID: 37795471 Free PMC article. Review.
-
Survival Analysis and Recurrence Patterns in 555 Patients with Colorectal Peritoneal Metastases Treated by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy.Ann Surg Oncol. 2024 Dec;31(13):8585-8595. doi: 10.1245/s10434-024-15942-1. Epub 2024 Aug 11. Ann Surg Oncol. 2024. PMID: 39128977
-
Comprehensive Treatment Algorithms of the Swiss Peritoneal Cancer Group for Peritoneal Cancer of Gastrointestinal Origin.Cancers (Basel). 2022 Sep 1;14(17):4275. doi: 10.3390/cancers14174275. Cancers (Basel). 2022. PMID: 36077810 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J Clin. 2018;68:394–424. - PubMed
-
- Thomassen I, van Gestel YR, Lemmens VE, de Hingh IH. Incidence, prognosis, and treatment options for patients with synchronous peritoneal carcinomatosis and liver metastases from colorectal origin. Dis Colon Rectum. 2013;56:1373–80. - PubMed
-
- McCormack PM, Burt ME, Bains MS, Martini N, Rusch VW, Ginsberg RJ. Lung resection for colorectal metastases. 10-year results. Arch Surg. 1992;127:1403–6. - PubMed
-
- van Gestel YR, de Hingh IH, van Herk-Sukel MP, van Erning FN, Beerepoot LV, Wijsman JH, et al. Patterns of metachronous metastases after curative treatment of colorectal cancer. Cancer Epidemiol. 2014;38:448–54. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
