

Insulin at 100 years - is rebalancing its action key to fighting obesity-related disease?
- PMID: 34841432
- PMCID: PMC8649170
- DOI: 10.1242/dmm.049340
Insulin at 100 years - is rebalancing its action key to fighting obesity-related disease?
Abstract
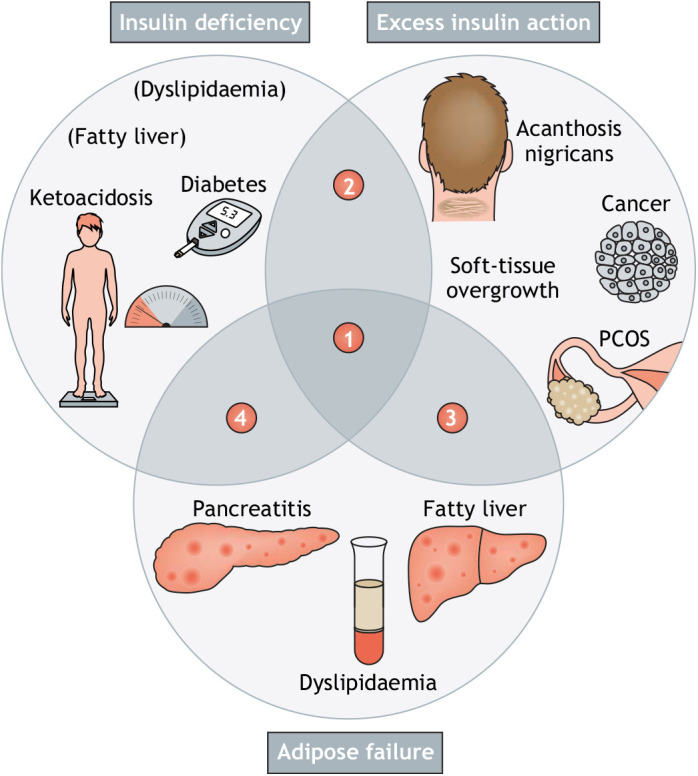
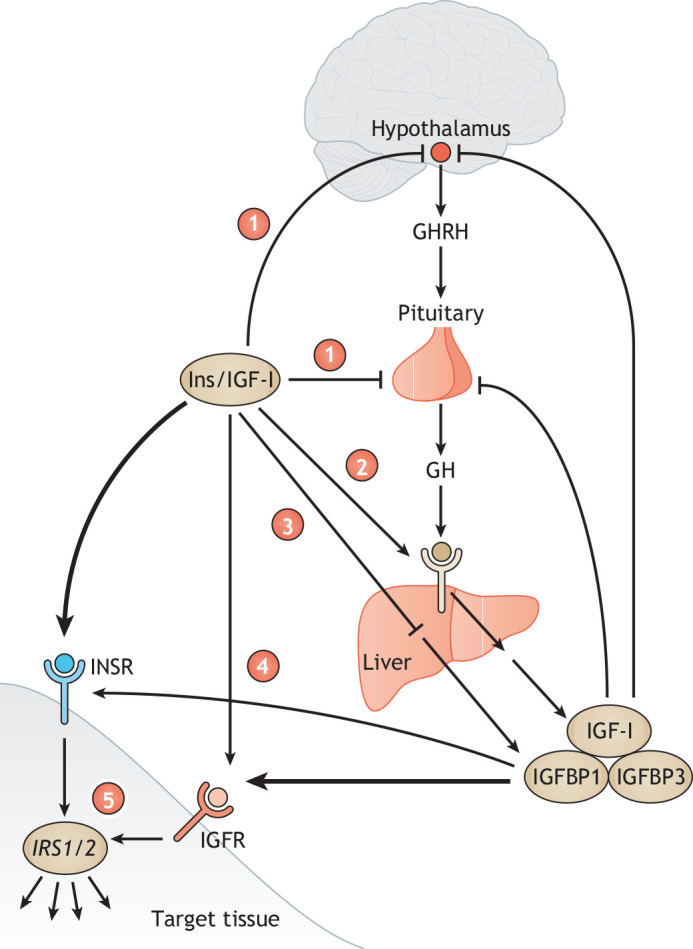
One hundred years ago, insulin was purified and administered to people with diabetes to lower blood glucose, suppress ketogenesis and save lives. A century later, insulin resistance (IR) lies at the heart of the obesity-related disease pandemic. Multiple observations attest that IR syndrome is an amalgamation of gain and loss of insulin action, suggesting that IR is a misnomer. This misapprehension is reinforced by shortcomings in common model systems and is particularly pronounced for the tissue growth disorders associated with IR. It is necessary to move away from conceptualisation of IR as a pure state of impaired insulin action and to appreciate that, in the long term, insulin can harm as well as cure. The mixed state of gain and loss of insulin action, and its relationship to perturbed insulin-like growth factor (IGF) action, should be interrogated more fully in models recapitulating human disease. Only then may the potential of rebalancing insulin action, rather than simply increasing global insulin signalling, finally be appreciated.
© 2021. Published by The Company of Biologists Ltd.
Conflict of interest statement
Competing interests The authors declare no competing or financial interests.
Figures

Similar articles
-
Diabetes and branched-chain amino acids: What is the link?J Diabetes. 2018 May;10(5):350-352. doi: 10.1111/1753-0407.12645. Epub 2018 Feb 13. J Diabetes. 2018. PMID: 29369529
-
Metabolism and insulin signaling in common metabolic disorders and inherited insulin resistance.Dan Med J. 2014 Jul;61(7):B4890. Dan Med J. 2014. PMID: 25123125 Review.
-
Cardiometabolic risk factors and insulin resistance in obese children and adolescents: relation to puberty.Pediatr Obes. 2015 Feb;10(1):37-44. doi: 10.1111/j.2047-6310.2013.00202.x. Epub 2013 Nov 13. Pediatr Obes. 2015. PMID: 24227418
-
[Obesity--insulin resistance--type 2 diabetes mellitus].Kardiol Pol. 2006 Oct;64(10 Suppl 6):S561-6. Kardiol Pol. 2006. PMID: 20527377 Review. Polish.
-
Metabolic alterations in adolescents with obstructive sleep apnea.Int J Pediatr Otorhinolaryngol. 2015 Dec;79(12):2368-73. doi: 10.1016/j.ijporl.2015.10.046. Epub 2015 Nov 3. Int J Pediatr Otorhinolaryngol. 2015. PMID: 26581829
Cited by
-
Insulin Resistance and Adrenal Androgen Synthesis Viewed Through a Monogenic Lens.J Clin Endocrinol Metab. 2022 Nov 23;107(11):e4326-e4327. doi: 10.1210/clinem/dgac475. J Clin Endocrinol Metab. 2022. PMID: 35961312 Free PMC article. No abstract available.
-
What lies beyond 100 years of insulin.Dis Model Mech. 2021 Nov 1;14(11):dmm049361. doi: 10.1242/dmm.049361. Epub 2021 Nov 9. Dis Model Mech. 2021. PMID: 34752619 Free PMC article.
References
-
- Bliss, M. (1982). The Discovery of Insulin: The Twenty-fifth Anniversary Edition. University of Toronto Press.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
