

Ten-year changes in plasma L-carnitine levels and risk of coronary heart disease
- PMID: 34799774
- PMCID: PMC9208674
- DOI: 10.1007/s00394-021-02713-x
Ten-year changes in plasma L-carnitine levels and risk of coronary heart disease
Abstract
Purpose: L-Carnitine is abundant in animal source foods, particularly red meat, and circulating L-carnitine may be related to the incidence of coronary heart disease (CHD). We investigated whether long-term changes in plasma L-carnitine over 10 years were associated with the CHD incidence and also examined joint associations of carnitine-rich red meat consumption and L-carnitine changes on the subsequent risk of CHD.
Methods: This prospective nested case-control study included 772 healthy women at baseline (386 incident CHD cases and 386 healthy controls). Plasma L-carnitine levels were measured both at the first (1989-90) and second blood collections (2000-02). Incident cases of CHD were prospectively followed from the date of the second blood collection through 2016.
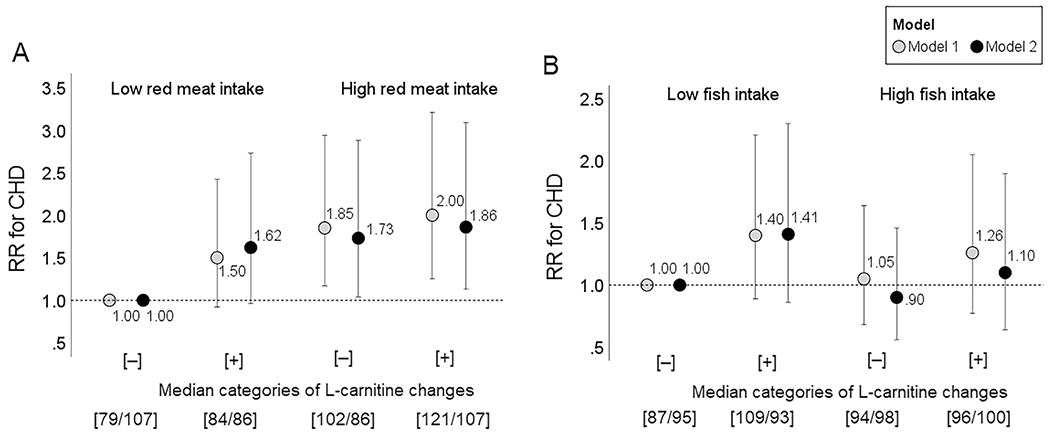
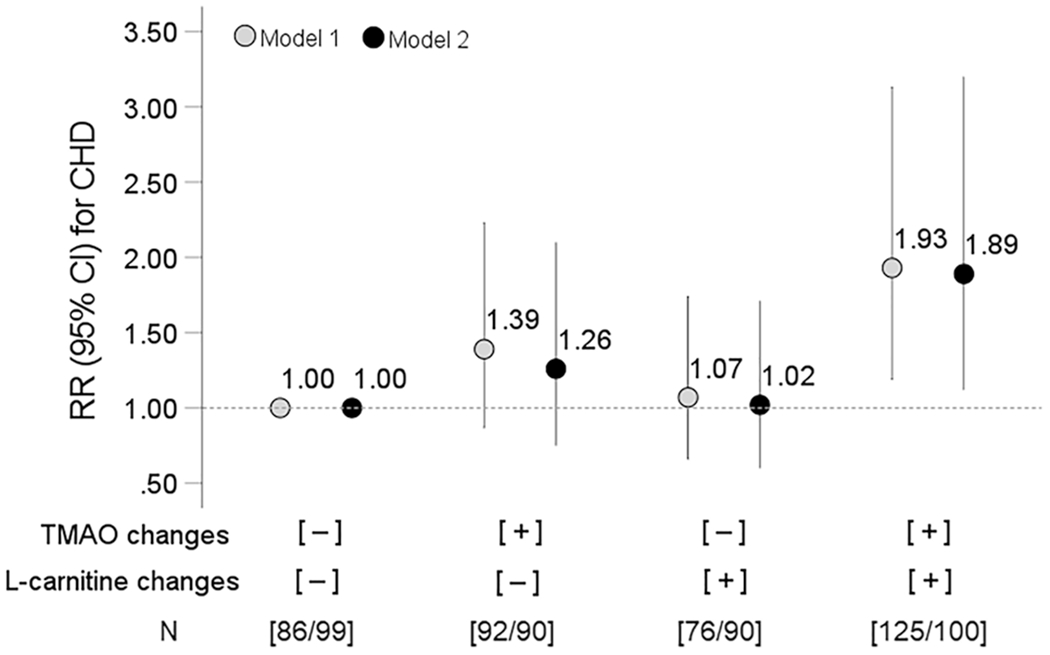
Results: Overall, a greater increase in L-carnitine from the first to the second time point was related to a higher risk of CHD, regardless of the initial L-carnitine levels (relative risk: 1.36 (95% CI 0.999, 1.84) per 1-SD increase). The 10-year changes in L-carnitine were positively associated with red meat consumption over time, and women with higher red meat intake (≥ 36 g/day) and with greater increases in L-carnitine had a 1.86 (95% CI 1.13, 3.09) times increased risk of CHD, as compared to those with lower red meat intake and lesser increases in L-carnitine.
Conclusion: Long-term increases in L-carnitine levels were associated with the subsequent incidence of CHD, especially among women with higher intake of red meat. Our results suggest the importance of atherogenic L-carnitine changes and dietary intakes over time in the prevention of CHD.
Keywords: Coronary heart disease; Diet; Gut microbiota-related metabolite; L-Carnitine; Risk; Trimethylamine N-oxide.
© 2021. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany.
Conflict of interest statement
Figures

Similar articles
-
Long-Term Changes in Gut Microbial Metabolite Trimethylamine N-Oxide and Coronary Heart Disease Risk.J Am Coll Cardiol. 2020 Feb 25;75(7):763-772. doi: 10.1016/j.jacc.2019.11.060. J Am Coll Cardiol. 2020. PMID: 32081286 Free PMC article.
-
Urinary Levels of Trimethylamine-N-Oxide and Incident Coronary Heart Disease: A Prospective Investigation Among Urban Chinese Adults.J Am Heart Assoc. 2019 Jan 8;8(1):e010606. doi: 10.1161/JAHA.118.010606. J Am Heart Assoc. 2019. PMID: 30606084 Free PMC article.
-
Red meat intake and risk of coronary heart disease among US men: prospective cohort study.BMJ. 2020 Dec 2;371:m4141. doi: 10.1136/bmj.m4141. BMJ. 2020. PMID: 33268459 Free PMC article.
-
Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: a systematic review and meta-analysis.Circulation. 2010 Jun 1;121(21):2271-83. doi: 10.1161/CIRCULATIONAHA.109.924977. Epub 2010 May 17. Circulation. 2010. PMID: 20479151 Free PMC article. Review.
-
Meat lipids, NaCl and carnitine: Do they unveil the conundrum of the association between red and processed meat intake and cardiovascular diseases?_Invited Review.Meat Sci. 2021 Jan;171:108278. doi: 10.1016/j.meatsci.2020.108278. Epub 2020 Aug 11. Meat Sci. 2021. PMID: 32861180 Review.
Cited by
-
Global Scientific Trends on Healthy Eating from 2002 to 2021: A Bibliometric and Visualized Analysis.Nutrients. 2023 Mar 17;15(6):1461. doi: 10.3390/nu15061461. Nutrients. 2023. PMID: 36986189 Free PMC article. Review.
-
Coronary heart disease and gut microbiota: A bibliometric and visual analysis from 2002 to 2022.Front Cardiovasc Med. 2022 Sep 8;9:949859. doi: 10.3389/fcvm.2022.949859. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36158832 Free PMC article.
-
Consumption of different types of meat and the risk of chronic limb-threatening ischemia: the Singapore Chinese Health Study.Nutr J. 2024 Sep 7;23(1):103. doi: 10.1186/s12937-024-00991-9. Nutr J. 2024. PMID: 39244535 Free PMC article.
-
Carnitine is a friend in HFpEF and foe in HFrEF.iScience. 2024 Sep 23;27(10):111018. doi: 10.1016/j.isci.2024.111018. eCollection 2024 Oct 18. iScience. 2024. PMID: 39429785 Free PMC article.
References
-
- Zununi Vahed S, Barzegari A, Zuluaga M, Letourneur D, Pavon-Djavid G (2018) Myocardial infarction and gut microbiota: An incidental connection. Pharmacol Res 129:308–317 - PubMed
-
- Zhu Q, Gao R, Zhang Y et al. (2018) Dysbiosis signatures of gut microbiota in coronary artery disease. Physiol Genomics 50:893–903 - PubMed
MeSH terms
Substances
Grants and funding
- HL071981/HL/NHLBI NIH HHS/United States
- R01 DK115679/DK/NIDDK NIH HHS/United States
- DK115679/DK/NIDDK NIH HHS/United States
- R01 DK091718/DK/NIDDK NIH HHS/United States
- Postdoctoral Fellowship for Research Abroad/Japan Society for the Promotion of Science
- DK091718/DK/NIDDK NIH HHS/United States
- P30 DK046200/DK/NIDDK NIH HHS/United States
- R21 HL126024/HL/NHLBI NIH HHS/United States
- S10 OD016346/OD/NIH HHS/United States
- S10OD016346/NH/NIH HHS/United States
- R01 HL071981/HL/NHLBI NIH HHS/United States
- R01 CA049449/CA/NCI NIH HHS/United States
- DK100383/DK/NIDDK NIH HHS/United States
- R21 TW010790/TW/FIC NIH HHS/United States
- 19POST34380035/American Heart Association
- HL126024/HL/NHLBI NIH HHS/United States
- R01 HL034594/HL/NHLBI NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- CA49449/CA/NCI NIH HHS/United States
- R01 DK100383/DK/NIDDK NIH HHS/United States
- rant-in-Aid for Scientific Research/Japan Society for the Promotion of Science
- R01 HL088521/HL/NHLBI NIH HHS/United States
- U01 CA049449/CA/NCI NIH HHS/United States
- DK46200/Boston Obesity Nutrition Research Center
LinkOut - more resources
Full Text Sources
