

SARS-CoV-2, COVID-19 and the Ageing Immune System
- PMID: 34746804
- PMCID: PMC8570568
- DOI: 10.1038/s43587-021-00114-7
SARS-CoV-2, COVID-19 and the Ageing Immune System
Abstract
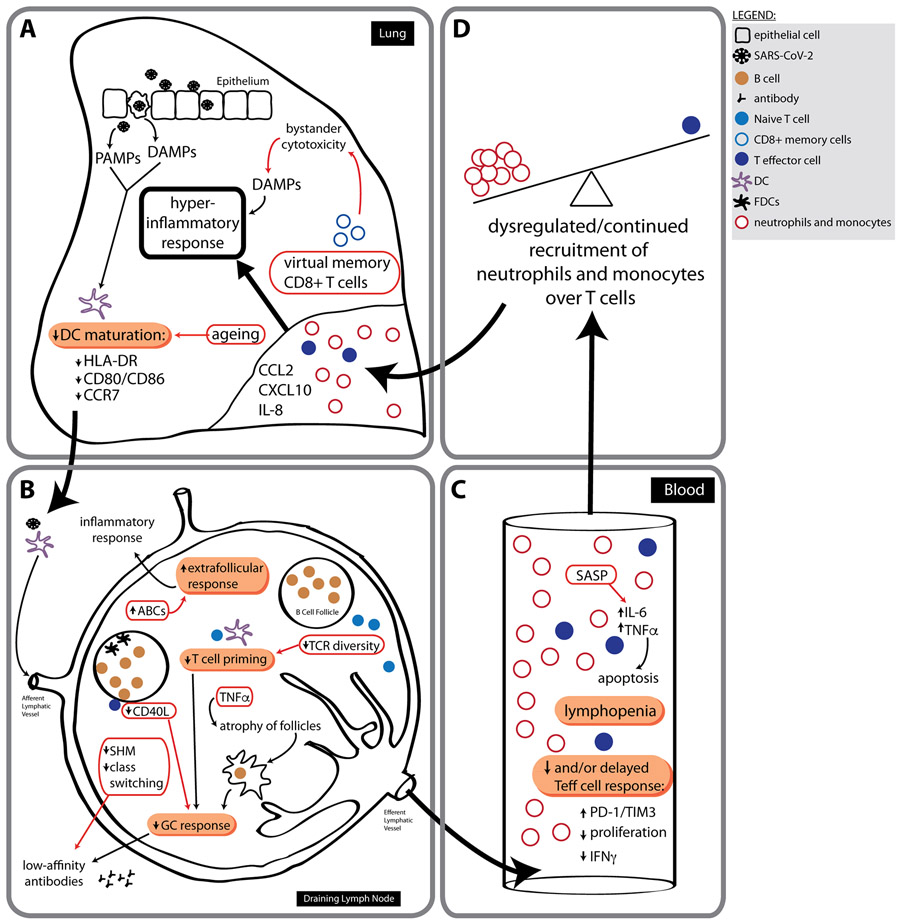
The coronavirus disease 2019 (COVID-19) pandemic is a global health threat with particular risk for severe disease and death in older adults and in adults with age-related metabolic and cardiovascular disease. Recent advances in the science of ageing have highlighted how ageing pathways control not only lifespan but also healthspan, the healthy years of life. Here, we discuss the ageing immune system and its ability to respond to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). We specifically focus on the intersect of severe COVID-19 and immunosenescence to highlight pathways that may be determinant for the risk of complications and death following infection with SARS-CoV-2. New or adapted therapeutics that target ageing-associated pathways may be important tools to reduce the burden of death and long-term disability caused by this pandemic. Proposed interventions aimed at immunosenescence could enhance immune function not only in the elderly but in susceptible younger individuals as well, ultimately improving complications of severe COVID-19 for all ages.
Figures
Similar articles
-
Immunosenescence and inflamm-ageing in COVID-19.Ageing Res Rev. 2023 Feb;84:101818. doi: 10.1016/j.arr.2022.101818. Epub 2022 Dec 11. Ageing Res Rev. 2023. PMID: 36516928 Free PMC article. Review.
-
Role of Senescence and Aging in SARS-CoV-2 Infection and COVID-19 Disease.Cells. 2021 Nov 30;10(12):3367. doi: 10.3390/cells10123367. Cells. 2021. PMID: 34943875 Free PMC article. Review.
-
Immunosenescence and COVID-19.Mech Ageing Dev. 2022 Jun;204:111672. doi: 10.1016/j.mad.2022.111672. Epub 2022 Apr 1. Mech Ageing Dev. 2022. PMID: 35378106 Free PMC article. Review.
-
I mmunosenescence and Inflammaging: Risk Factors of Severe COVID-19 in Older People.Front Immunol. 2020 Oct 27;11:579220. doi: 10.3389/fimmu.2020.579220. eCollection 2020. Front Immunol. 2020. PMID: 33193377 Free PMC article. Review.
-
COVID-19 and Crosstalk With the Hallmarks of Aging.J Gerontol A Biol Sci Med Sci. 2020 Sep 16;75(9):e34-e41. doi: 10.1093/gerona/glaa149. J Gerontol A Biol Sci Med Sci. 2020. PMID: 32544216 Free PMC article. Review.
Cited by
-
Heterologous DNA-prime/protein-boost immunization with a monomeric SARS-CoV-2 spike antigen redundantizes the trimeric receptor-binding domain structure to induce neutralizing antibodies in old mice.Front Immunol. 2023 Sep 11;14:1231274. doi: 10.3389/fimmu.2023.1231274. eCollection 2023. Front Immunol. 2023. PMID: 37753087 Free PMC article.
-
The Impact of Immune System Aging on Infectious Diseases.Microorganisms. 2024 Apr 11;12(4):775. doi: 10.3390/microorganisms12040775. Microorganisms. 2024. PMID: 38674719 Free PMC article. Review.
-
Circulating multimeric immune complexes contribute to immunopathology in COVID-19.Nat Commun. 2022 Sep 26;13(1):5654. doi: 10.1038/s41467-022-32867-z. Nat Commun. 2022. PMID: 36163132 Free PMC article.
-
Neutrophil heterogeneity and aging: implications for COVID-19 and wound healing.Front Immunol. 2023 Nov 28;14:1201651. doi: 10.3389/fimmu.2023.1201651. eCollection 2023. Front Immunol. 2023. PMID: 38090596 Free PMC article. Review.
-
Infection, pathology and interferon treatment of the SARS-CoV-2 Omicron BA.1 variant in juvenile, adult and aged Syrian hamsters.Cell Mol Immunol. 2022 Dec;19(12):1392-1399. doi: 10.1038/s41423-022-00923-9. Epub 2022 Oct 18. Cell Mol Immunol. 2022. PMID: 36258005 Free PMC article.
References
-
- Yoshikawa TT Epidemiology and unique aspects of aging and infectious diseases. Clin Infect Dis 30, 931–933 (2000). - PubMed
-
- Goodwin K, Viboud C & Simonsen L Antibody response to influenza vaccination in the elderly: a quantitative review. Vaccine 24, 1159–1169 (2006). - PubMed
-
- Melegaro A & Edmunds WJ The 23-valent pneumococcal polysaccharide vaccine. Part I. Efficacy of PPV in the elderly: a comparison of meta-analyses. Eur J Epidemiol 19, 353–363 (2004). - PubMed
-
- Wolters B, Junge U, Dziuba S & Roggendorf M Immunogenicity of combined hepatitis A and B vaccine in elderly persons. Vaccine 21, 3623–3628 (2003). - PubMed
-
- Kaml M, et al. Booster vaccination in the elderly: their success depends on the vaccine type applied earlier in life as well as on pre-vaccination antibody titers. Vaccine 24, 6808–6811 (2006). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
