

COVID-19 and Indirect Liver Injury: A Narrative Synthesis of the Evidence
- PMID: 34722191
- PMCID: PMC8516829
- DOI: 10.14218/JCTH.2020.00140
COVID-19 and Indirect Liver Injury: A Narrative Synthesis of the Evidence
Abstract
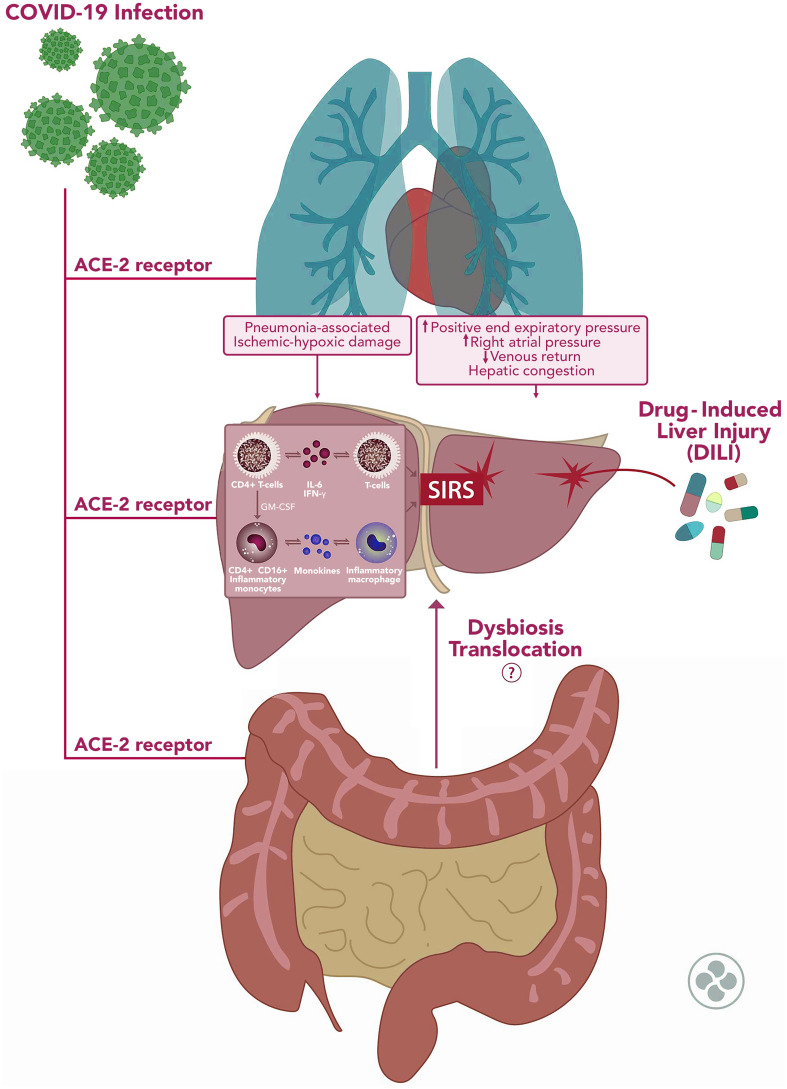
The liver is frequently affected by severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2) infection. The most common manifestations are mildly elevated alanine aminotransferase and aspartate aminotransferase, with a prevalence of 16-53% among patients. Cases with severe coronavirus disease 2019 (COVID-19) seem to have higher rates of acute liver dysfunction, and the presence of abnormal liver tests at admission signifies a higher risk of severe disease during hospitalization. Patients with chronic liver diseases also have a higher risk of severe disease and mortality (mainly seen in patients with metabolic-associated fatty liver disease). Several pathways of damage have been proposed in the liver involvement of COVID-19 patients; although, the end-cause is most likely multifactorial. Abnormal liver tests have been attributed to the expression of angiotensin-converting enzyme 2 receptors in SARS-CoV-2 infection. This enzyme is expressed widely in cholangiocytes and less in hepatocytes. Other factors attributed to liver damage include drug-induced liver injury, uncontrolled release of proinflammatory molecules ("cytokine storm"), pneumonia-associated hypoxia, and direct damage by the infection. Hepatic steatosis, vascular thrombosis, fibrosis, and inflammatory features (including Kupffer cell hyperplasia) are the most common liver histopathological findings in deceased COVID-19 patients, suggesting important indirect mechanisms of liver damage. In this translational medicine-based narrative review, we summarize the current data on the possible indirect mechanisms involved in liver damage due to COVID-19, the histopathological findings, and the impact of these mechanisms in patients with chronic liver disease.
Keywords: COVID-19; Liver hepatitis; Liver injury; Novel coronavirus; SARS-CoV-2.
© 2021 Authors.
Conflict of interest statement
The authors have no conflict of interests related to this publication.
Figures
Similar articles
-
SARS-CoV-2 infection of the liver directly contributes to hepatic impairment in patients with COVID-19.J Hepatol. 2020 Oct;73(4):807-816. doi: 10.1016/j.jhep.2020.05.002. Epub 2020 May 11. J Hepatol. 2020. PMID: 32437830 Free PMC article.
-
Association between COVID-19 and chronic liver disease: Mechanism, diagnosis, damage, and treatment.World J Virol. 2023 Jan 25;12(1):22-29. doi: 10.5501/wjv.v12.i1.22. World J Virol. 2023. PMID: 36743657 Free PMC article. Review.
-
Liver dysfunction as a cytokine storm manifestation and prognostic factor for severe COVID-19.World J Hepatol. 2021 Dec 27;13(12):2005-2012. doi: 10.4254/wjh.v13.i12.2005. World J Hepatol. 2021. PMID: 35070004 Free PMC article. Review.
-
SARS-CoV-2 induced liver injury: Incidence, risk factors, impact on COVID-19 severity and prognosis in different population groups.World J Gastroenterol. 2023 Apr 28;29(16):2397-2432. doi: 10.3748/wjg.v29.i16.2397. World J Gastroenterol. 2023. PMID: 37179584 Free PMC article. Review.
-
COVID-19 and liver injury: Pathophysiology, risk factors, outcome and management in special populations.World J Hepatol. 2023 Apr 27;15(4):441-459. doi: 10.4254/wjh.v15.i4.441. World J Hepatol. 2023. PMID: 37206656 Free PMC article. Review.
Cited by
-
Impact of non-alcoholic fatty liver disease on coronavirus disease 2019: A systematic review.World J Hepatol. 2024 Aug 27;16(8):1185-1198. doi: 10.4254/wjh.v16.i8.1185. World J Hepatol. 2024. PMID: 39221098 Free PMC article.
-
Effects of COVID-19 on the Liver and Mortality in Patients with SARS-CoV-2 Pneumonia Caused by Delta and Non-Delta Variants: An Analysis in a Single Centre.Pharmaceuticals (Basel). 2023 Dec 19;17(1):3. doi: 10.3390/ph17010003. Pharmaceuticals (Basel). 2023. PMID: 38275989 Free PMC article.
-
An Updated Systematic Review and Meta-Analysis of the Association between the De Ritis Ratio and Disease Severity and Mortality in Patients with COVID-19.Life (Basel). 2023 Jun 5;13(6):1324. doi: 10.3390/life13061324. Life (Basel). 2023. PMID: 37374107 Free PMC article. Review.
-
COVID-19-Associated Liver Injury.Hepat Med. 2023 Feb 21;15:1-9. doi: 10.2147/HMER.S384108. eCollection 2023. Hepat Med. 2023. PMID: 36852138 Free PMC article. Review.
-
Frontiers and hotspots evolution in cytokine storm: A bibliometric analysis from 2004 to 2022.Heliyon. 2024 May 10;10(10):e30955. doi: 10.1016/j.heliyon.2024.e30955. eCollection 2024 May 30. Heliyon. 2024. PMID: 38774317 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous