

Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses
- PMID: 34717822
- PMCID: PMC8600124
- DOI: 10.1016/S2213-8587(21)00263-1
Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses
Retraction in
-
Retraction and republication-Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses.Lancet Diabetes Endocrinol. 2024 Jan;12(1):8. doi: 10.1016/S2213-8587(23)00364-9. Epub 2023 Dec 1. Lancet Diabetes Endocrinol. 2024. PMID: 38048795 Free PMC article. No abstract available.
Retracted and republished in
-
Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses.Lancet Diabetes Endocrinol. 2024 Jan;12(1):e2-e11. doi: 10.1016/S2213-8587(23)00287-5. Epub 2023 Dec 1. Lancet Diabetes Endocrinol. 2024. PMID: 38048800 Free PMC article.
Expression of concern in
-
Expression of Concern-Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses.Lancet Diabetes Endocrinol. 2023 Sep;11(9):634. doi: 10.1016/S2213-8587(23)00198-5. Epub 2023 Jul 13. Lancet Diabetes Endocrinol. 2023. PMID: 37454668 Free PMC article. No abstract available.
Abstract
Background: Randomised trials of vitamin D supplementation for cardiovascular disease and all-cause mortality have generally reported null findings. However, generalisability of results to individuals with low vitamin D status is unclear. We aimed to characterise dose-response relationships between 25-hydroxyvitamin D (25[OH]D) concentrations and risk of coronary heart disease, stroke, and all-cause mortality in observational and Mendelian randomisation frameworks.
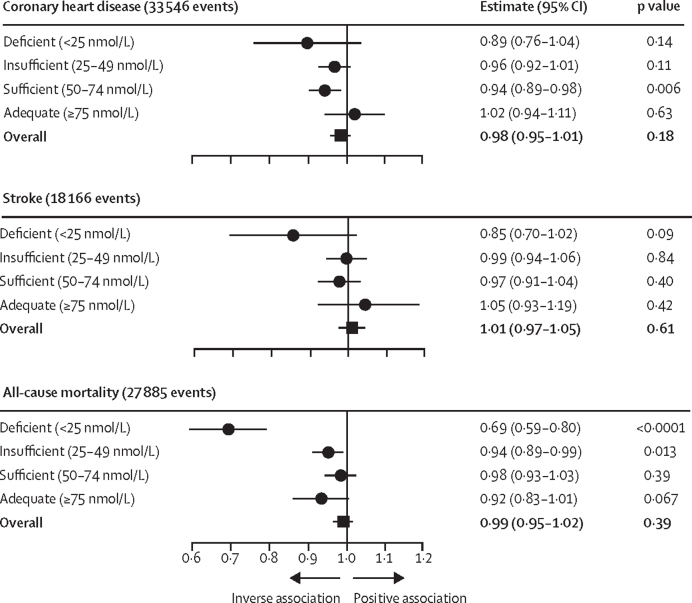
Methods: Observational analyses were undertaken using data from 33 prospective studies comprising 500 962 individuals with no known history of coronary heart disease or stroke at baseline. Mendelian randomisation analyses were performed in four population-based cohort studies (UK Biobank, EPIC-CVD, and two Copenhagen population-based studies) comprising 386 406 middle-aged individuals of European ancestries, including 33 546 people who developed coronary heart disease, 18 166 people who had a stroke, and 27 885 people who died. Primary outcomes were coronary heart disease, defined as fatal ischaemic heart disease (International Classification of Diseases 10th revision code I20-I25) or non-fatal myocardial infarction (I21-I23); stroke, defined as any cerebrovascular disease (I60-I69); and all-cause mortality.
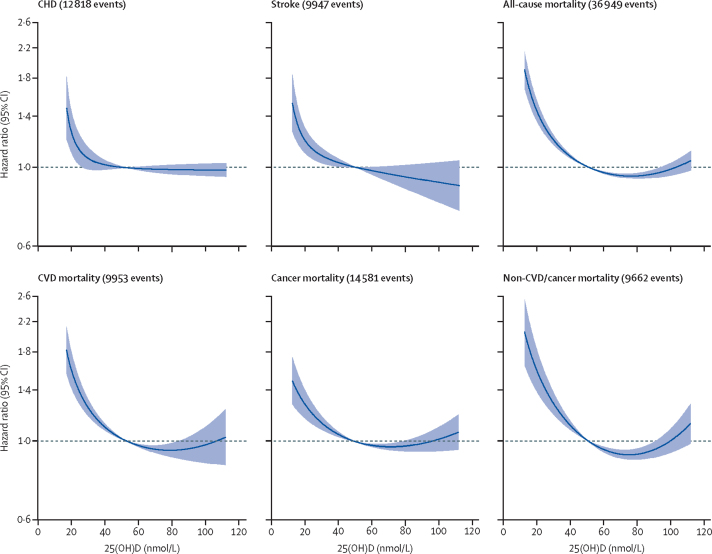
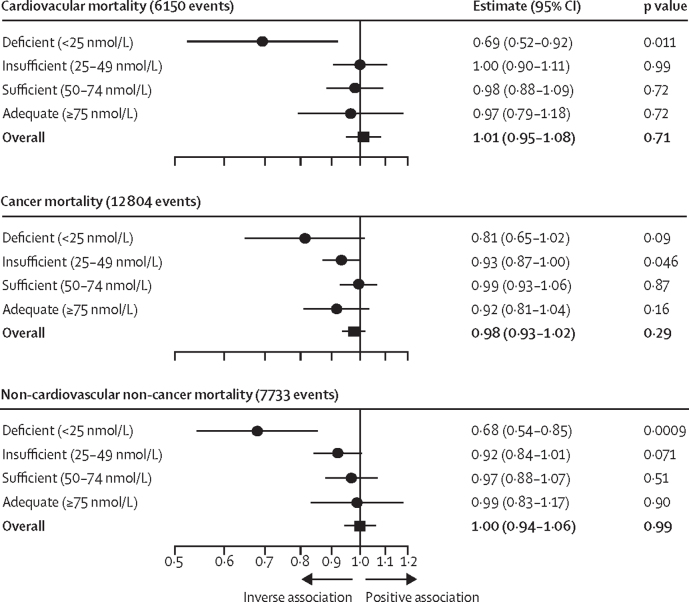
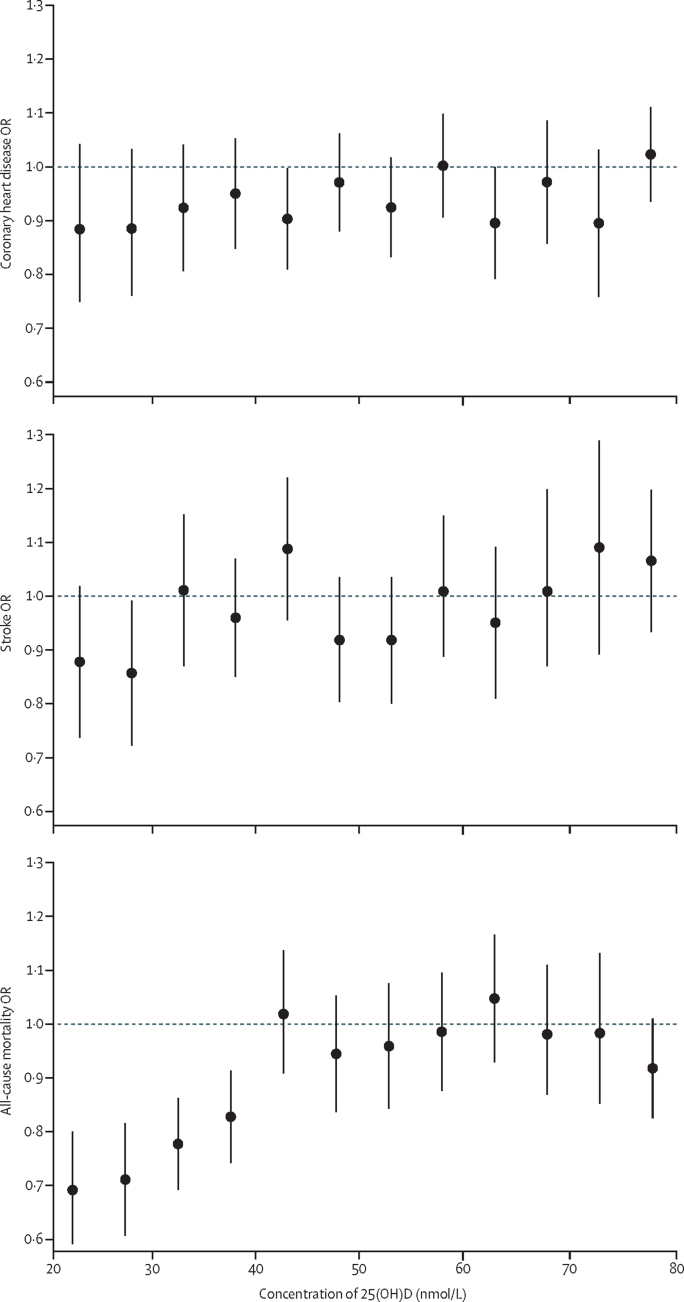
Findings: Observational analyses suggested inverse associations between incident coronary heart disease, stroke, and all-cause mortality outcomes with 25(OH)D concentration at low 25(OH)D concentrations. In population-wide genetic analyses, there were no associations of genetically-predicted 25(OH)D with coronary heart disease, stroke, or all-cause mortality. However, for the participants with vitamin D deficiency (25[OH]D concentration <25 nmol/L), genetic analyses provided strong evidence for an inverse association with all-cause mortality (odds ratio [OR] per 10 nmol/L increase in genetically-predicted 25[OH]D concentration 0·69 [95% CI 0·59-0·80]; p<0·0001) and non-significant inverse associations for stroke (0·85 [0·70-1·02], p=0·09) and coronary heart disease (0·89 [0·76-1·04]; p=0·14). A finer stratification of participants found inverse associations between genetically-predicted 25(OH)D concentrations and all-cause mortality up to around 40 nmol/L.
Interpretation: Stratified Mendelian randomisation analyses suggest a causal relationship between 25(OH)D concentrations and mortality for individuals with low vitamin D status. Our findings have implications for the design of vitamin D supplementation trials, and potential disease prevention strategies.
Funding: British Heart Foundation, Medical Research Council, National Institute for Health Research, Health Data Research UK, Cancer Research UK, and International Agency for Research on Cancer.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests ASB reports grants outside of this work from AstraZeneca, Biogen, BioMarin, Bioverativ, Merck, Novartis, Pfizer, and Sanofi and personal fees from Novartis. JD reports grants, personal fees, and non-financial support from Merck Sharp & Dohme, grants, personal fees, and non-financial support from Novartis, grants from Pfizer, and grants from AstraZeneca outside the submitted work. YÇ reports personal fees from Boehringer Ingelheim, AstraZeneca, and Sanofi Genzyme outside the submitted work. BGN reports consultancies and talks sponsored by AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Esperion, and Silence Therapeutics outside submitted work. MA is now an employee of AstraZeneca. DG is employed part-time by Novo Nordisk. PW reports grant income from Roche Diagnostics, AstraZeneca, Boehringer Ingelheim, and Novartis outside the submitted work. NS reports personal fees from Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Merck Sharp and Dohme, Novartis, Novo Nordisk, Pfizer, and Sanofi, and grant funding paid to his institution from AstraZeneca, Boehringer Ingelheim, and Roche Diagnostics. All other authors declare no competing interests.
Figures
Comment in
-
WITHDRAWN: Targeting of vitamin D supplementation to individuals with deficiency.Lancet Diabetes Endocrinol. 2021 Dec;9(12):803-804. doi: 10.1016/S2213-8587(21)00282-5. Epub 2021 Oct 28. Lancet Diabetes Endocrinol. 2021. Retraction in: Lancet Diabetes Endocrinol. 2024 Jan;12(1):8. doi: 10.1016/S2213-8587(23)00364-9. PMID: 34717823 Retracted. No abstract available.
-
Dose-response relationships for vitamin D and all-cause mortality - Authors' reply.Lancet Diabetes Endocrinol. 2022 Mar;10(3):158-159. doi: 10.1016/S2213-8587(22)00015-8. Lancet Diabetes Endocrinol. 2022. PMID: 35202588 No abstract available.
-
Dose-response relationships for vitamin D and all-cause mortality.Lancet Diabetes Endocrinol. 2022 Mar;10(3):158. doi: 10.1016/S2213-8587(22)00013-4. Lancet Diabetes Endocrinol. 2022. PMID: 35202589 No abstract available.
-
Mendelian randomisation and vitamin D: the importance of model assumptions.Lancet Diabetes Endocrinol. 2023 Jan;11(1):14-15. doi: 10.1016/S2213-8587(22)00342-4. Lancet Diabetes Endocrinol. 2023. PMID: 36528344 No abstract available.
-
Mendelian randomisation and vitamin D: the importance of model assumptions.Lancet Diabetes Endocrinol. 2023 Jan;11(1):14. doi: 10.1016/S2213-8587(22)00345-X. Lancet Diabetes Endocrinol. 2023. PMID: 36528345 No abstract available.
-
Mendelian randomisation and vitamin D: the importance of model assumptions - Authors' reply.Lancet Diabetes Endocrinol. 2023 Jan;11(1):15-16. doi: 10.1016/S2213-8587(22)00344-8. Lancet Diabetes Endocrinol. 2023. PMID: 36528346 No abstract available.
Similar articles
-
Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses.Lancet Diabetes Endocrinol. 2024 Jan;12(1):e2-e11. doi: 10.1016/S2213-8587(23)00287-5. Epub 2023 Dec 1. Lancet Diabetes Endocrinol. 2024. PMID: 38048800 Free PMC article.
-
No evidence that genetically reduced 25-hydroxyvitamin D is associated with increased risk of ischaemic heart disease or myocardial infarction: a Mendelian randomization study.Int J Epidemiol. 2015 Apr;44(2):651-61. doi: 10.1093/ije/dyv078. Epub 2015 May 16. Int J Epidemiol. 2015. PMID: 25981321
-
Vitamin D and brain health: an observational and Mendelian randomization study.Am J Clin Nutr. 2022 Aug 4;116(2):531-540. doi: 10.1093/ajcn/nqac107. Am J Clin Nutr. 2022. PMID: 35451454 Free PMC article.
-
The relationship of vitamin D status to risk of cardiovascular disease and mortality.Dan Med J. 2015 Feb;62(2):B5008. Dan Med J. 2015. PMID: 25634511 Review.
-
Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: a meta-analysis of prospective studies.Circ Cardiovasc Qual Outcomes. 2012 Nov;5(6):819-29. doi: 10.1161/CIRCOUTCOMES.112.967604. Epub 2012 Nov 13. Circ Cardiovasc Qual Outcomes. 2012. PMID: 23149428 Free PMC article. Review.
Cited by
-
Calcifediol (25OH Vitamin D3) Deficiency: A Risk Factor from Early to Old Age.Nutrients. 2022 Mar 10;14(6):1168. doi: 10.3390/nu14061168. Nutrients. 2022. PMID: 35334824 Free PMC article. Review.
-
Dietary Recommendations for Post-COVID-19 Syndrome.Nutrients. 2022 Mar 20;14(6):1305. doi: 10.3390/nu14061305. Nutrients. 2022. PMID: 35334962 Free PMC article. Review.
-
Genetic Polymorphism of NQO1 Influences Susceptibility to Coronary Heart Disease in a Chinese Population: A Cross-Sectional Study and Meta-Anaylsis.Pharmgenomics Pers Med. 2023 Sep 11;16:825-833. doi: 10.2147/PGPM.S420874. eCollection 2023. Pharmgenomics Pers Med. 2023. PMID: 37720192 Free PMC article.
-
The Impact of Baseline 25-Hydroxyvitamin D Level and Gestational Age on Prenatal Vitamin D Supplementation to Prevent Offspring Asthma or Recurrent Wheezing.Am J Clin Nutr. 2023 Jun;117(6):1342-1352. doi: 10.1016/j.ajcnut.2023.04.019. Epub 2023 Apr 17. Am J Clin Nutr. 2023. PMID: 37075847 Free PMC article. Clinical Trial.
-
Identification and single-base gene-editing functional validation of a cis-EPO variant as a genetic predictor for EPO-increasing therapies.Am J Hum Genet. 2022 Sep 1;109(9):1638-1652. doi: 10.1016/j.ajhg.2022.08.004. Am J Hum Genet. 2022. PMID: 36055212 Free PMC article.
References
-
- Zittermann A, Ernst JB, Prokop S, et al. Effect of vitamin D on all-cause mortality in heart failure (EVITA): a 3-year randomized clinical trial with 4000 IU vitamin D daily. Eur Heart J. 2017;38:2279–2286. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01HC95160/HL/NHLBI NIH HHS/United States
- N01HC95163/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- R01 AR035584/AR/NIAMS NIH HHS/United States
- U01 AG042124/AG/NIA NIH HHS/United States
- N01HC95168/HL/NHLBI NIH HHS/United States
- R01 AG005407/AG/NIA NIH HHS/United States
- N01HC95159/HL/NHLBI NIH HHS/United States
- N01HC95167/HL/NHLBI NIH HHS/United States
- 16896/CRUK_/Cancer Research UK/United Kingdom
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- MC_UU_00006/1/MRC_/Medical Research Council/United Kingdom
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- UL1 TR000128/TR/NCATS NIH HHS/United States
- R01 AR035583/AR/NIAMS NIH HHS/United States
- G0800270/MRC_/Medical Research Council/United Kingdom
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- N01HC95169/HL/NHLBI NIH HHS/United States
- N01HC95164/HL/NHLBI NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- R01 AG027576/AG/NIA NIH HHS/United States
- N01HC95162/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- N01HC95165/HL/NHLBI NIH HHS/United States
- N01HC95161/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- G1000143/MRC_/Medical Research Council/United Kingdom
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- MC_UU_00002/7/MRC_/Medical Research Council/United Kingdom
- CH/1996001/9454/BHF_/British Heart Foundation/United Kingdom
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- P30 DK035816/DK/NIDDK NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- R01 AR035582/AR/NIAMS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- U01 AG027810/AG/NIA NIH HHS/United States
- R01 AG005394/AG/NIA NIH HHS/United States
- MC_UU_12015/5/MRC_/Medical Research Council/United Kingdom
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- MC_UU_00006/3/MRC_/Medical Research Council/United Kingdom
- N01HC95166/HL/NHLBI NIH HHS/United States
- R01 HL096875/HL/NHLBI NIH HHS/United States
- U01 AG042143/AG/NIA NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
- R01 AG027574/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
