

The Neutrophil-to-Lymphocyte Ratio Is an Important Indicator Predicting In-Hospital Death in AMI Patients
- PMID: 34616780
- PMCID: PMC8488114
- DOI: 10.3389/fcvm.2021.706852
The Neutrophil-to-Lymphocyte Ratio Is an Important Indicator Predicting In-Hospital Death in AMI Patients
Abstract
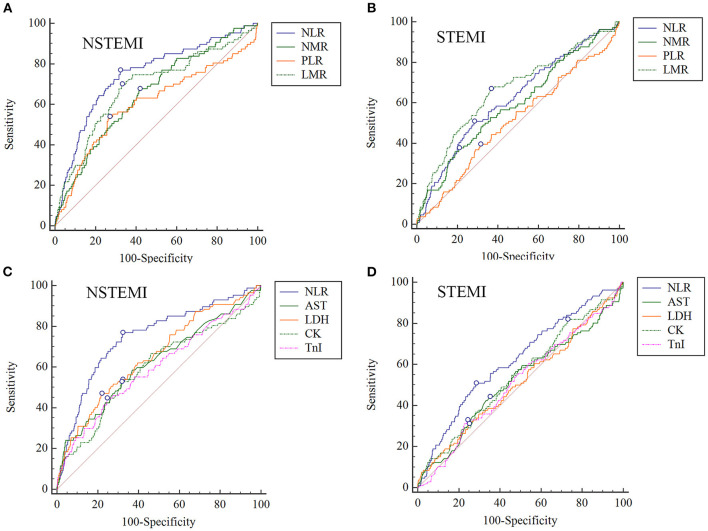
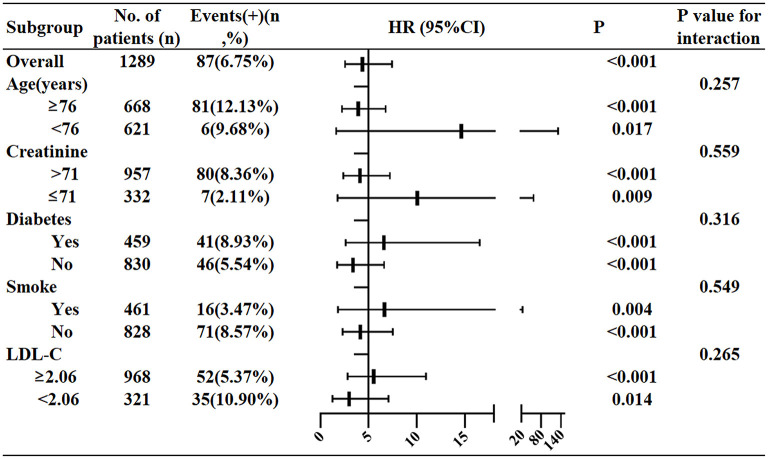
Objective: To explore the role of neutrophil-to-lymphocyte ratio (NLR) in predicting the short-term prognosis of NSTEMI and STEMI. Methods: This study was a single-center, retrospective and observational study. 2618 patients including 1289 NSTMI and 1329 STEMI patients were enrolled from June 2013 to February 2018 in Zhongda Hospital, Southeast University. The demographic information, clinical characteristics, medical history, laboratory examination, treatment, and outcome of individuals at admission and during hospitalization were extracted from the electronic medical record system. Outcome was defined as the all-cause death during hospitalization. Results: (1) In the NSTEMI group, the ability of NLR in predicting in-hospital death (AUC = 0.746) was higher than the neutrophil-monocyte ratio (NMR) (AUC = 0.654), the platelet-lymphocyte ratio (PLR) (AUC = 0.603) and the lymphocyte-monocyte ratio (LMR) (AUC = 0.685), and also higher than AST (AUC = 0.621), CK (AUC = 0.595), LDH (AUC = 0.653) and TnI (AUC = 0.594). The AUC of NLR in the STEMI group was only 0.621. (2) The optimal cut-off value of NLR in NSTEMI group was 5.509 (Youden index = 0.447, sensitivity = 77.01%, specificity = 67.72%). After adjusting variables including age, sex, diabetes history, smoking history, LDL-C and Cr, the logistic regression showed that the patients with NLR>5.509 had higher hazard risk of death (HR4.356; 95%CI 2.552-7.435; P < 0.001) than the patients with NLR ≤ 5.509. (3) Stratification analysis showed that the in-hospital mortality of patients with NLR > 5.509 was 14.611-fold higher than those with NLR ≤ 5.509 in patients aged <76, much higher than the ratio in patients aged ≥ 76. For patients with creatinine levels ≤ 71, the in-hospital death risk in high NLR group was 10.065-fold higher than in low NLR group (95%CI 1.761-57.514, P = 0.009), while the HR was only 4.117 in patients with creatinine levels > 71. The HR in patients with or without diabetes were 6.586 and 3.375, respectively. The HR in smoking or no smoking patients were 6.646 and 4.145, respectively. The HR in patients with LDL-C ≥ 2.06 or <2.06 were 5.526 and 2.967 respectively. Conclusion: Compared to NMR, PLR, and LMR, NLR had the best ability in predicting in-hospital death after NSTEMI. Age, creatinine, LDL-C, diabetes and smoking history were all important factors affecting the predictive efficiency in NSTEMI. NLR had the limited predictive ability in STEMI.
Keywords: acute myocardial infarction (AMI); biomarker; blood routine examination; neutrophil to lymphocyte ratio; prognosis.
Copyright © 2021 Ji, Liu, Guo, Zhang, Su, Carvalho, Qu, Zuo, Yao, Lin and Ma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio are Important Indicators for Predicting in-Hospital Death in Elderly AMI Patients.J Inflamm Res. 2023 May 15;16:2051-2061. doi: 10.2147/JIR.S411086. eCollection 2023. J Inflamm Res. 2023. PMID: 37215380 Free PMC article.
-
Diagnostic and prognostic role of neutrophil/lymphocyte ratio, platelet/lymphocyte ratio, and lymphocyte/monocyte ratio in patients with osteosarcoma.Jt Dis Relat Surg. 2021;32(2):489-496. doi: 10.52312/jdrs.2021.79775. Epub 2021 Jun 11. Jt Dis Relat Surg. 2021. PMID: 34145828 Free PMC article.
-
The relationship between platelet-to-lymphocyte ratio and pulmonary embolism severity in acute pulmonary embolism.Int Angiol. 2019 Feb;38(1):4-9. doi: 10.23736/S0392-9590.18.04028-2. Epub 2019 Jan 4. Int Angiol. 2019. PMID: 30618227
-
Prognostic Value of Neutrophil:Lymphocyte and Platelet:Lymphocyte Ratios for 28-Day Mortality of Patients with AECOPD.Int J Gen Med. 2021 Jun 25;14:2839-2848. doi: 10.2147/IJGM.S312045. eCollection 2021. Int J Gen Med. 2021. PMID: 34211292 Free PMC article.
-
The Role of Neutrophil-to-Lymphocyte Ratio in Predicting Outcomes of Acute Organophosphorus Poisoning: A Comprehensive Review.Cureus. 2024 May 22;16(5):e60854. doi: 10.7759/cureus.60854. eCollection 2024 May. Cureus. 2024. PMID: 38910647 Free PMC article. Review.
Cited by
-
Elevated ApoB/apoA-1 is Associated with in-Hospital Mortality in Elderly Patients with Acute Myocardial Infarction.Diabetes Metab Syndr Obes. 2023 Nov 3;16:3501-3512. doi: 10.2147/DMSO.S433876. eCollection 2023. Diabetes Metab Syndr Obes. 2023. PMID: 37942174 Free PMC article.
-
High neutrophil-to-lymphocyte ratio is associated with cancer therapy-related cardiovascular toxicity in high-risk cancer patients under immune checkpoint inhibitor therapy.Clin Res Cardiol. 2024 Feb;113(2):301-312. doi: 10.1007/s00392-023-02327-9. Epub 2023 Nov 13. Clin Res Cardiol. 2024. PMID: 37955712 Free PMC article.
-
Clinical features and in-hospital mortality predictors of concurrent cardio-cerebral infarction: insights from a dual-center retrospective study.Front Neurol. 2024 Oct 8;15:1465144. doi: 10.3389/fneur.2024.1465144. eCollection 2024. Front Neurol. 2024. PMID: 39474370 Free PMC article.
-
Impact of lactate dehydrogenase on prognosis of patients undergoing cardiac surgery.BMC Cardiovasc Disord. 2022 Sep 10;22(1):404. doi: 10.1186/s12872-022-02848-7. BMC Cardiovasc Disord. 2022. PMID: 36088306 Free PMC article.
-
The Prognostic Role of the Neutrophil-to-Lymphocytes Ratio in the Most Frequent Cardiovascular Diseases: An Update.Life (Basel). 2024 Aug 7;14(8):985. doi: 10.3390/life14080985. Life (Basel). 2024. PMID: 39202727 Free PMC article. Review.
References
-
- Chinese Society of Cardiology of Chinese Medical A Editorial Board of Chinese Journal of C . 2019 Chinese Society of Cardiology (CSC) guidelines for the diagnosis and management of patients with ST-segment elevation myocardial infarction. Zhonghua xin xue guan bing za zhi. (2019) 47:766–83. 10.3760/cma.j.issn.0253-3758.2019.10.003 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials