

T-Lymphocyte Subsets Alteration, Infection and Renal Outcome in Advanced Chronic Kidney Disease
- PMID: 34568395
- PMCID: PMC8458643
- DOI: 10.3389/fmed.2021.742419
T-Lymphocyte Subsets Alteration, Infection and Renal Outcome in Advanced Chronic Kidney Disease
Abstract
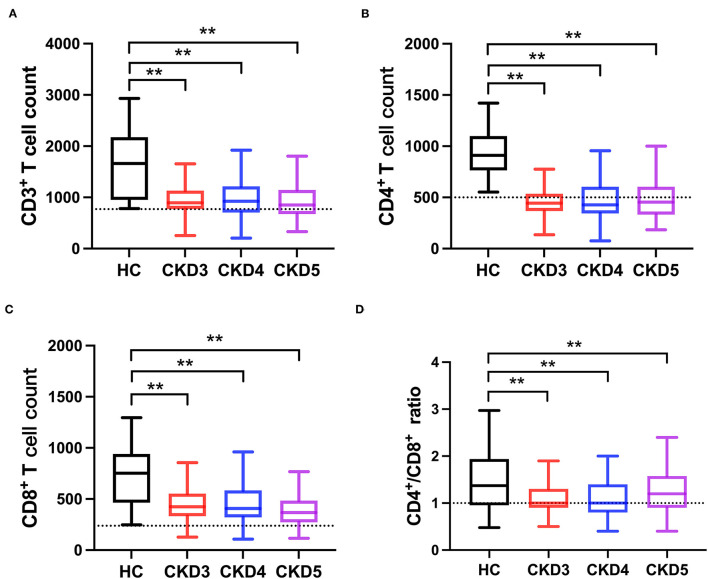
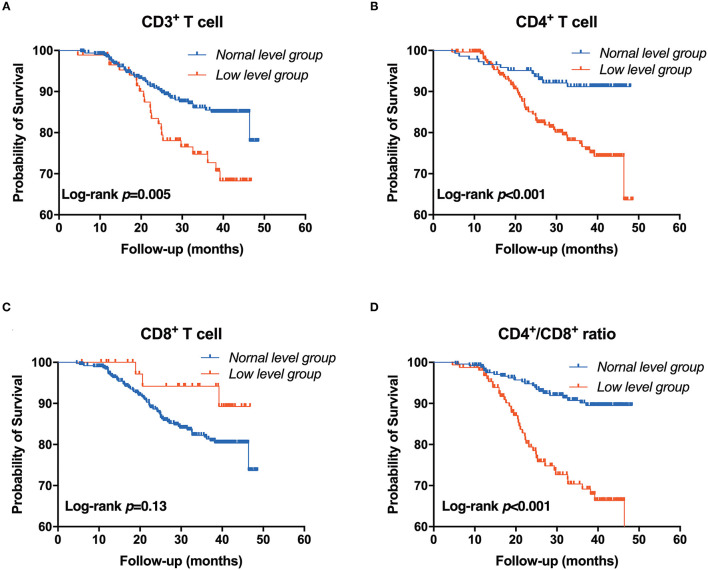
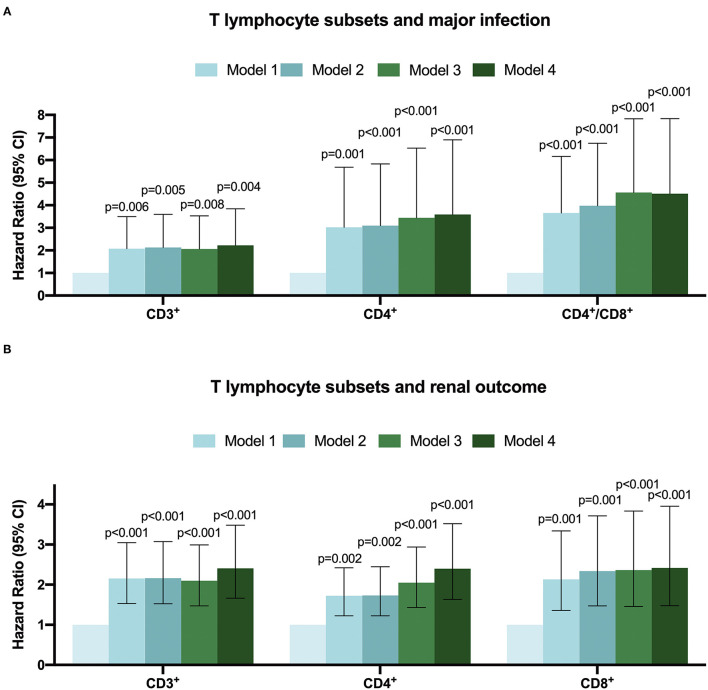
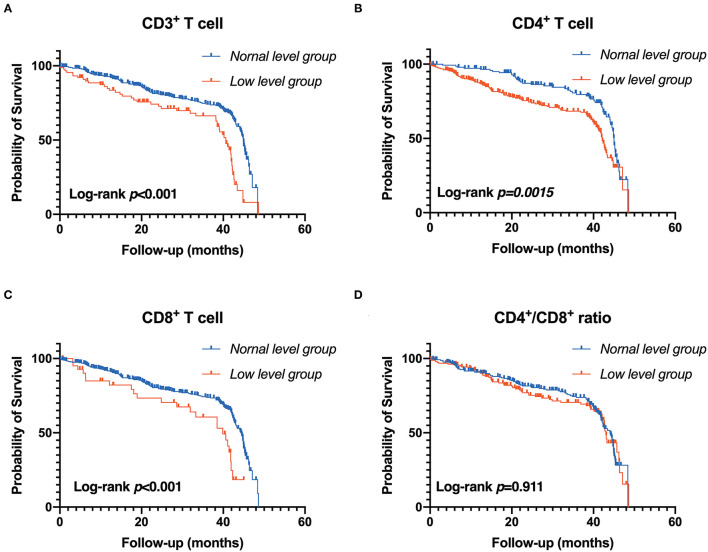
Background: T-lymphocyte subsets reflect patients' immune status and are associated with adverse outcomes in various diseases. However, the association between T-lymphocyte subsets and major infection and renal outcome in chronic kidney disease (CKD) patients has not been well-addressed. Methods: Patients diagnosed with stage 3-5 of non-dialysis CKD were recruited, and healthy subjects were selected as the controls. T-lymphocyte subsets (CD3+, CD4+, CD8+) were detected by flow cytometry, and the CD4+/CD8+ T cell ratio was then calculated. Patients were divided into the normal-level group and the low-level group according to the clinical reference value. The primary outcomes were the major infection and renal outcome. Results: A total of 410 CKD patients were enrolled; the average age was 47.25 years. Compared to the healthy controls, the level of CD3+, CD4+, CD8+ T cells, and the CD4+/CD8+ T cell ratio were significantly decreased in CKD patients (p < 0.05). During the median follow-up of 2.56 (quartile interval 1.24-3.46) years, major infections occurred in 15.10% of the CKD patients. The incidence of infection was significantly higher in the low-level group of CD3+, CD4+ T cells, and CD4+/CD8+ T cell ratio compared with the normal level groups. Kaplan-Meier analysis showed that the lower level of CD3+, CD4+ T cells, and CD4+/CD8+T cell ratio is associated with a greater risk of infection. Cox regression analysis further confirmed that low CD3+, CD4+ T cells, and CD4+/CD8+ T cell ratio were independent risk factors of infection in CKD patients. Moreover, during the follow-up, renal events occurred in 37.50% of patients. Kaplan-Meier analysis indicated that low levels of CD3+, CD4+, and CD8+ T cells are significantly associated with renal outcome in CKD patients. Cox regression analysis showed that low level of CD3+ T cells (HR = 2.407, 95% CI: 1.664-3.482, p < 0.001), CD4+ T cells (HR = 2.397, 95% CI: 1.633-3.518, p < 0.001) and CD8+ T cells (HR = 2.416, 95% CI: 1.476-3.955, p < 0.001) were independent risk factors for renal outcome after multivariable-adjusted. Conclusion: CKD patients had a defect in T-lymphocyte subpopulation. T-lymphocyte subsets were closely associated with infection and renal outcome in CKD patients. Suggesting T-lymphocyte subsets are independent predictors of infection and renal outcome in CKD patients.
Keywords: T-lymphocyte; chronic kidney disease; infection; renal outcome; risk factors.
Copyright © 2021 Xiong, Qiao, Yu, Huang, Yang, He and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Evaluation of the clinical significance of lymphocyte subsets and myeloid suppressor cells in patients with renal carcinoma.Discov Oncol. 2024 Sep 30;15(1):512. doi: 10.1007/s12672-024-01405-2. Discov Oncol. 2024. PMID: 39347882 Free PMC article.
-
[Association of traumatic severity with change in lymphocyte subsets in the early stage after trauma].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013 Aug;25(8):489-92. doi: 10.3760/cma.j.issn.2095-4352.2013.08.010. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013. PMID: 24021046 Chinese.
-
Analysis of T-lymphocyte subsets and risk factors in children with tuberculosis.Tuberculosis (Edinb). 2024 May;146:102496. doi: 10.1016/j.tube.2024.102496. Epub 2024 Feb 20. Tuberculosis (Edinb). 2024. PMID: 38401266
-
Prognostic value of peripheral blood T lymphocyte subsets in clear cell renal cell carcinoma.Transl Androl Urol. 2021 Jan;10(1):326-335. doi: 10.21037/tau-20-1066. Transl Androl Urol. 2021. PMID: 33532321 Free PMC article.
-
[Deep lung--cellular reaction to HIV].Rev Port Pneumol. 2007 Mar-Apr;13(2):175-212. Rev Port Pneumol. 2007. PMID: 17492233 Review. Portuguese.
Cited by
-
Gut-immune axis and cardiovascular risk in chronic kidney disease.Clin Kidney J. 2023 Dec 13;17(1):sfad303. doi: 10.1093/ckj/sfad303. eCollection 2024 Jan. Clin Kidney J. 2023. PMID: 38229879 Free PMC article. Review.
-
Machine learning-based investigation of the relationship between immune status and left ventricular hypertrophy in patients with end-stage kidney disease.Front Cardiovasc Med. 2023 May 18;10:1187965. doi: 10.3389/fcvm.2023.1187965. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37273870 Free PMC article.
-
Multivariate canonical correlation analysis identifies additional genetic variants for chronic kidney disease.NPJ Syst Biol Appl. 2024 Mar 9;10(1):28. doi: 10.1038/s41540-024-00350-8. NPJ Syst Biol Appl. 2024. PMID: 38459044 Free PMC article.
-
Expansion of Double-Negative T Cells in Patients before Liver Transplantation Correlates with Post-Transplant Infections.J Clin Med. 2022 Jun 17;11(12):3502. doi: 10.3390/jcm11123502. J Clin Med. 2022. PMID: 35743569 Free PMC article.
-
Risk Factors of Arteriovenous Fistula Stenosis of Patients with Maintenance Hemodialysis.Evid Based Complement Alternat Med. 2022 Nov 3;2022:2968122. doi: 10.1155/2022/2968122. eCollection 2022. Evid Based Complement Alternat Med. 2022. Retraction in: Evid Based Complement Alternat Med. 2023 Jul 19;2023:9819702. doi: 10.1155/2023/9819702 PMID: 36387371 Free PMC article. Retracted.
References
-
- Townsend RR, Anderson AH, Chirinos JA, Feldman HI, Grunwald JE, Nessel L, et al. . Association of pulse wave velocity with chronic kidney disease progression and mortality: findings from the CRIC study (Chronic Renal Insufficiency Cohort). Hypertension. (2018) 71:1101–7. 10.1161/HYPERTENSIONAHA.117.10648 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials