

Antibody and cellular therapies for treatment of covid-19: a living systematic review and network meta-analysis
- PMID: 34556486
- PMCID: PMC8459162
- DOI: 10.1136/bmj.n2231
Antibody and cellular therapies for treatment of covid-19: a living systematic review and network meta-analysis
Abstract
Objective: To evaluate the efficacy and safety of antiviral antibody therapies and blood products for the treatment of novel coronavirus disease 2019 (covid-19).
Design: Living systematic review and network meta-analysis, with pairwise meta-analysis for outcomes with insufficient data.
Data sources: WHO covid-19 database, a comprehensive multilingual source of global covid-19 literature, and six Chinese databases (up to 21 July 2021).
Study selection: Trials randomising people with suspected, probable, or confirmed covid-19 to antiviral antibody therapies, blood products, or standard care or placebo. Paired reviewers determined eligibility of trials independently and in duplicate.
Methods: After duplicate data abstraction, we performed random effects bayesian meta-analysis, including network meta-analysis for outcomes with sufficient data. We assessed risk of bias using a modification of the Cochrane risk of bias 2.0 tool. The certainty of the evidence was assessed using the grading of recommendations assessment, development, and evaluation (GRADE) approach. We meta-analysed interventions with ≥100 patients randomised or ≥20 events per treatment arm.
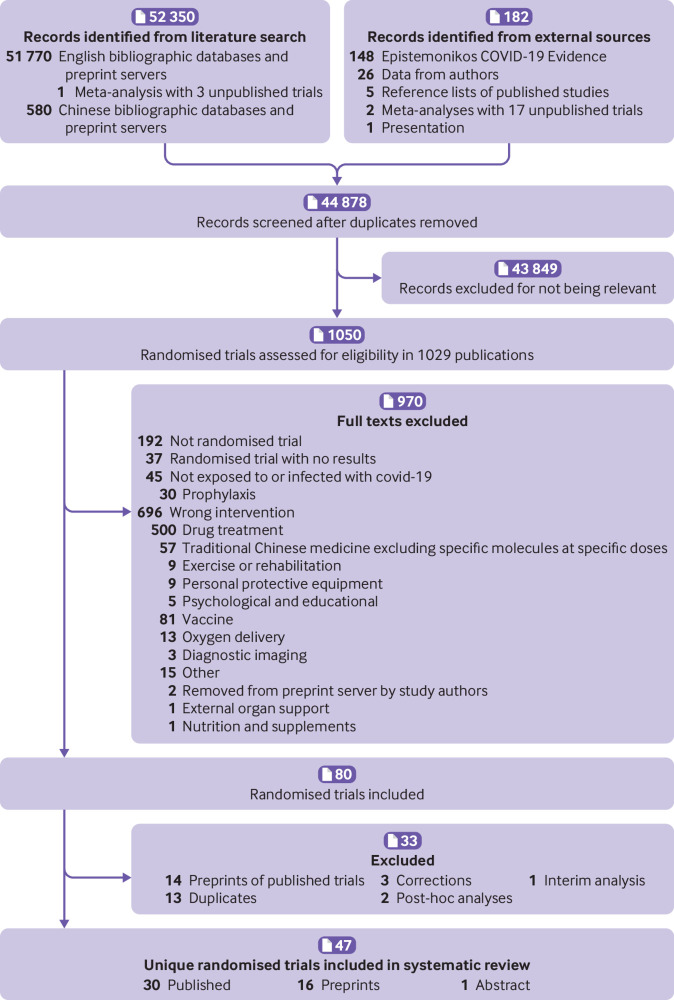
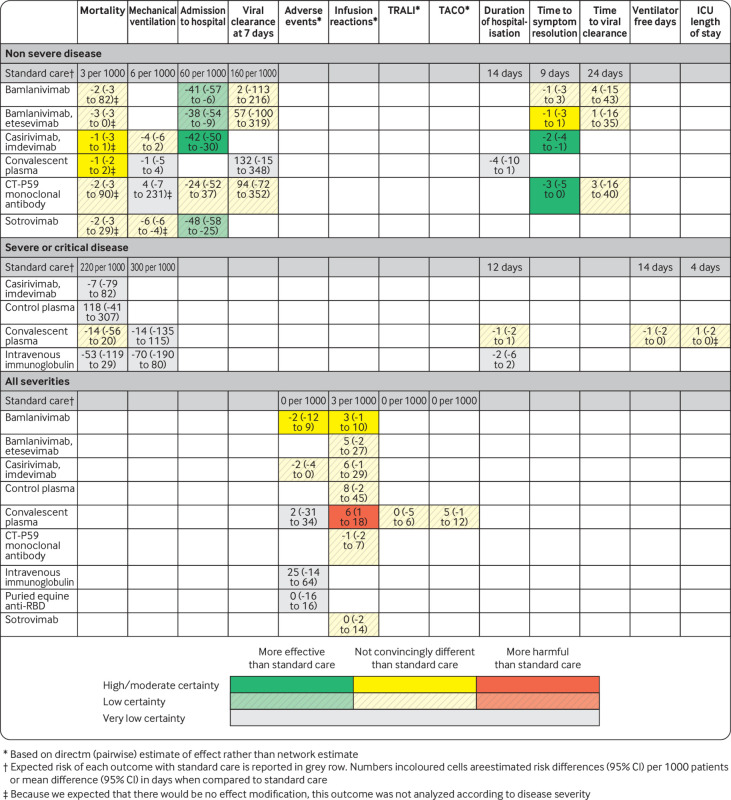
Results: As of 21 July 2021, we identified 47 trials evaluating convalescent plasma (21 trials), intravenous immunoglobulin (IVIg) (5 trials), umbilical cord mesenchymal stem cells (5 trials), bamlanivimab (4 trials), casirivimab-imdevimab (4 trials), bamlanivimab-etesevimab (2 trials), control plasma (2 trials), peripheral blood non-haematopoietic enriched stem cells (2 trials), sotrovimab (1 trial), anti-SARS-CoV-2 IVIg (1 trial), therapeutic plasma exchange (1 trial), XAV-19 polyclonal antibody (1 trial), CT-P59 monoclonal antibody (1 trial) and INM005 polyclonal antibody (1 trial) for the treatment of covid-19. Patients with non-severe disease randomised to antiviral monoclonal antibodies had lower risk of hospitalisation than those who received placebo: casirivimab-imdevimab (odds ratio (OR) 0.29 (95% CI 0.17 to 0.47); risk difference (RD) -4.2%; moderate certainty), bamlanivimab (OR 0.24 (0.06 to 0.86); RD -4.1%; low certainty), bamlanivimab-etesevimab (OR 0.31 (0.11 to 0.81); RD -3.8%; low certainty), and sotrovimab (OR 0.17 (0.04 to 0.57); RD -4.8%; low certainty). They did not have an important impact on any other outcome. There was no notable difference between monoclonal antibodies. No other intervention had any meaningful effect on any outcome in patients with non-severe covid-19. No intervention, including antiviral antibodies, had an important impact on any outcome in patients with severe or critical covid-19, except casirivimab-imdevimab, which may reduce mortality in patients who are seronegative.
Conclusion: In patients with non-severe covid-19, casirivimab-imdevimab probably reduces hospitalisation; bamlanivimab-etesevimab, bamlanivimab, and sotrovimab may reduce hospitalisation. Convalescent plasma, IVIg, and other antibody and cellular interventions may not confer any meaningful benefit.
Systematic review registration: This review was not registered. The protocol established a priori is included as a data supplement.
Funding: This study was supported by the Canadian Institutes of Health Research (grant CIHR- IRSC:0579001321).
Readers' note: This article is a living systematic review that will be updated to reflect emerging evidence. Interim updates and additional study data will be posted on our website (www.covid19lnma.com).
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Canadian Institutes of Health Research for the submitted work; ML reports personal fees and non-financial support from Sanofi, grants and personal fees from Seqirus, personal fees from Pfizer, and personal fees from Medicago outside the submitted work, and is a co-investigator on ACT randomised trial of covid-19 therapy; LG reports grants from Ministry of Science and Technology of China outside the submitted work.
Figures
Similar articles
-
SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19.Cochrane Database Syst Rev. 2021 Sep 2;9(9):CD013825. doi: 10.1002/14651858.CD013825.pub2. Cochrane Database Syst Rev. 2021. PMID: 34473343 Free PMC article. Review.
-
SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19.Cochrane Database Syst Rev. 2022 Jun 17;6(6):CD014945. doi: 10.1002/14651858.CD014945.pub2. Cochrane Database Syst Rev. 2022. PMID: 35713300 Free PMC article. Review.
-
Drug treatments for covid-19: living systematic review and network meta-analysis.BMJ. 2020 Jul 30;370:m2980. doi: 10.1136/bmj.m2980. BMJ. 2020. Update in: BMJ. 2020 Sep 11;370:m3536. doi: 10.1136/bmj.m3536. Update in: BMJ. 2020 Dec 17;371:m4852. doi: 10.1136/bmj.m4852. Update in: BMJ. 2021 Mar 31;372:n858. doi: 10.1136/bmj.n858. PMID: 32732190 Free PMC article. Updated.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: a rapid review.Cochrane Database Syst Rev. 2020 May 14;5(5):CD013600. doi: 10.1002/14651858.CD013600. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Jul 10;7:CD013600. doi: 10.1002/14651858.CD013600.pub2. PMID: 32406927 Free PMC article. Updated.
Cited by
-
Prophylaxis against covid-19: living systematic review and network meta-analysis.BMJ. 2021 Apr 26;373:n949. doi: 10.1136/bmj.n949. BMJ. 2021. PMID: 33903131 Free PMC article.
-
Intravenous immunoglobulin for treatment of hospitalized COVID-19 patients: an evidence mapping and meta-analysis.Inflammopharmacology. 2024 Feb;32(1):335-354. doi: 10.1007/s10787-023-01398-4. Epub 2023 Dec 14. Inflammopharmacology. 2024. PMID: 38097885 Review.
-
Real-world experience of monoclonal antibodies in mild-to-moderate COVID-19 patients at a tertiary care center.Med J Armed Forces India. 2023 May 18;80(Suppl 1):S180-4. doi: 10.1016/j.mjafi.2023.03.006. Online ahead of print. Med J Armed Forces India. 2023. PMID: 37360888
-
Hyperimmune immunoglobulin for people with COVID-19.Cochrane Database Syst Rev. 2023 Jan 26;1(1):CD015167. doi: 10.1002/14651858.CD015167.pub2. Cochrane Database Syst Rev. 2023. PMID: 36700518 Free PMC article. Review.
-
The efficiency of convalescent plasma in COVID-19 patients: A systematic review and meta-analysis of randomized controlled clinical trials.Front Immunol. 2022 Jul 28;13:964398. doi: 10.3389/fimmu.2022.964398. eCollection 2022. Front Immunol. 2022. PMID: 35967398 Free PMC article.
References
-
- Johns Hopkins University. Coronavirus resource center. 2020. https://coronavirus.jhu.edu/map.html.
-
- Cytel. Global coronavirus COVID-19 clinical trial tracker. 2020. https://www.covid19-trials.com/.
-
- Mair-Jenkins J, Saavedra-Campos M, Baillie JK, et al. Convalescent Plasma Study Group . The effectiveness of convalescent plasma and hyperimmune immunoglobulin for the treatment of severe acute respiratory infections of viral etiology: a systematic review and exploratory meta-analysis. J Infect Dis 2015;211:80-90. . 10.1093/infdis/jiu396 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous