

Diagnosis of "cribriform" prostatic adenocarcinoma: an interobserver reproducibility study among urologic pathologists with recommendations
- PMID: 34522463
- PMCID: PMC8414383
Diagnosis of "cribriform" prostatic adenocarcinoma: an interobserver reproducibility study among urologic pathologists with recommendations
Abstract
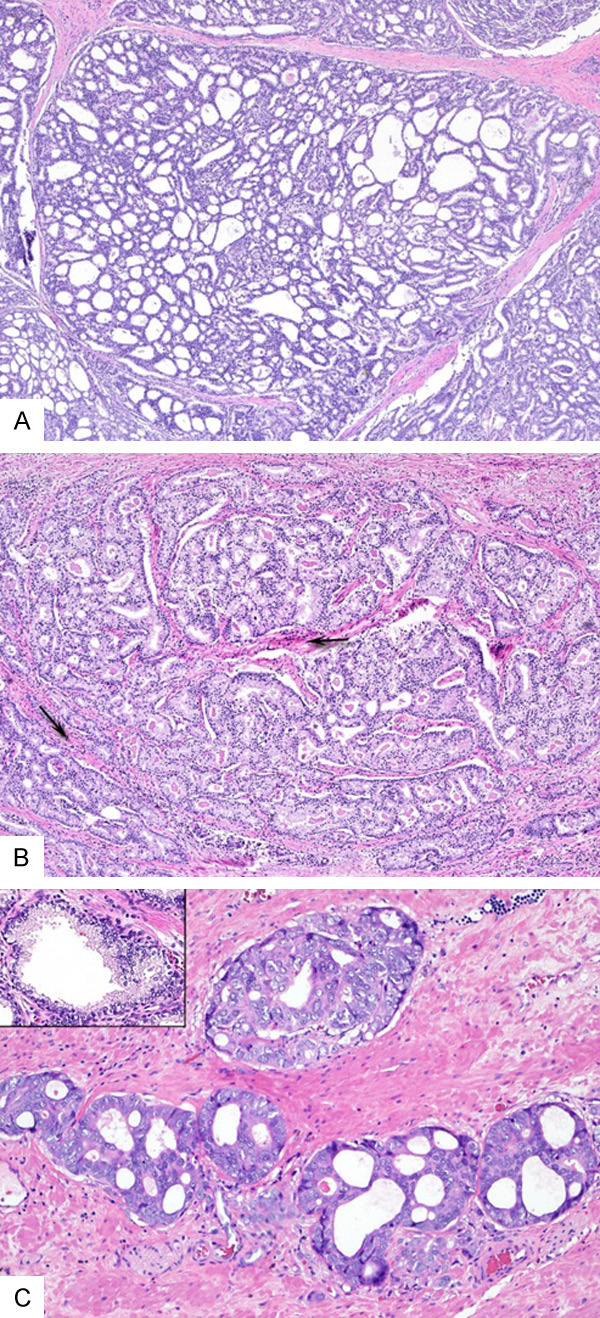
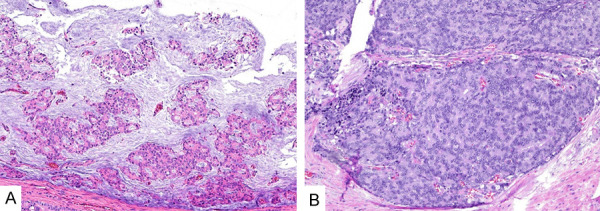
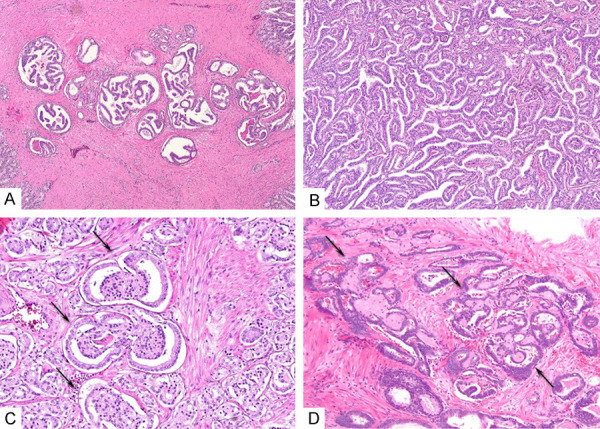
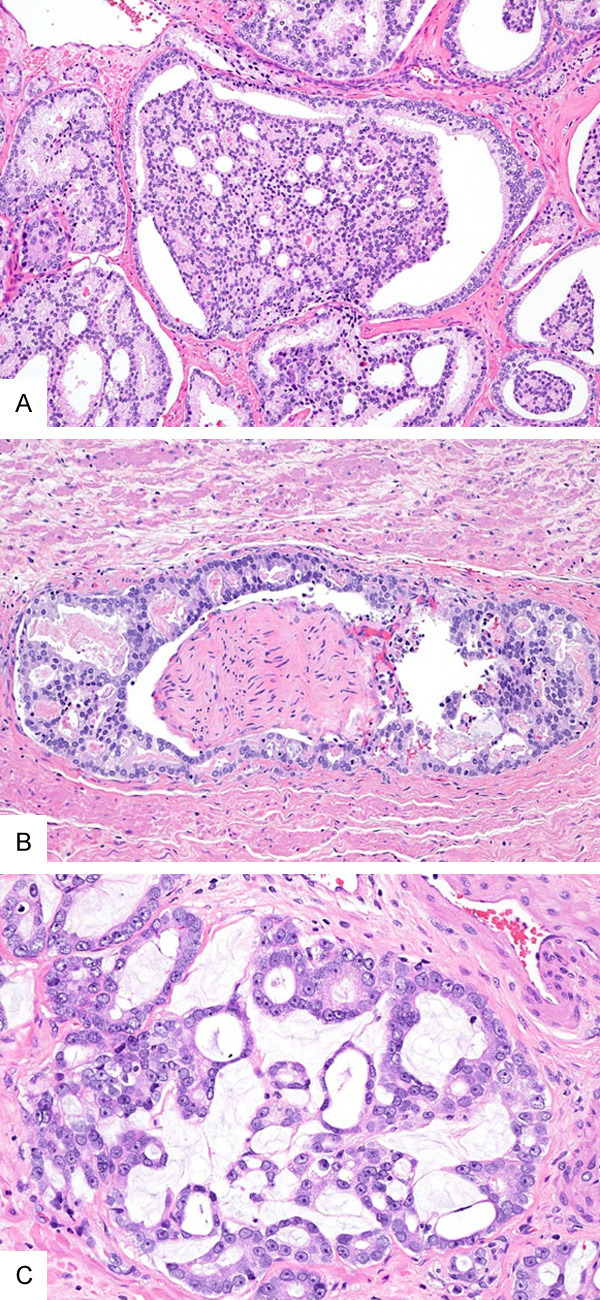
Accurate diagnosis of cribriform Gleason pattern 4 (CrP4) prostate adenocarcinoma (PCa) is important due to its independent association with adverse clinical outcomes and as a growing body of evidence suggests that it impacts clinical decision making in PCa management. To identify reproducible features for diagnosis of CrP4, we assessed interobserver agreement among 27 experienced urologic pathologists of 60 digital images from 44 radical prostatectomies (RP) that represented a broad spectrum of potential CrP4. The following morphologic features were correlated with the consensus diagnosis (defined as 75% agreement) for each image: partial vs. transluminal glandular bridging, intraglandular stroma, <12 vs. ≥12 lumina, well vs. poorly formed lumina, mucin (mucinous fibroplasia, extravasation, or extracellular pool), size (compared to benign glands and number of lumina), number of attachments with gland border by tumor cells forming a "glomeruloid-like" pattern, a clear luminal space along the periphery of gland occupying <50% of glandular circumference, central nerve, dense (cell mass occupying >50% of luminal space) vs. loose, and regular vs. irregular contour. Interobserver reproducibility for the overall diagnostic agreement was fair (k=0.40). Large CrP4 had better agreement (k=0.49) compared to small CrP4 (k=0.40). Transluminal bridging, dense cellular proliferation, a clear luminal space along the periphery of gland occupying <50% of gland circumference, lack of intraglandular mucin, and lack of contact between the majority of intraglandular cells with stroma were significantly associated with consensus for CrP4. In contrast, partial bridging, majority of intraglandular cells in contact with stroma, mucinous fibroplasia, only one attachment to the gland border by tumor cells forming a "glomeruloid-like" pattern, and a clear luminal space along the periphery of gland accounting for >50% of the glandular circumference were associated with consensus against CrP4. In summary, we identified reproducible morphological features for and against CrP4 diagnosis, which could be used to refine and standardize the diagnostic criteria for CrP4.
Keywords: Prostate adenocarcinoma; consensus; cribriform; gleason grade; grade group; reproducibility.
AJCR Copyright © 2021.
Conflict of interest statement
None.
Figures
Similar articles
-
Diagnosis of Gleason pattern 5 prostate adenocarcinoma on core needle biopsy: an interobserver reproducibility study among urologic pathologists.Am J Surg Pathol. 2015 Sep;39(9):1242-9. doi: 10.1097/PAS.0000000000000442. Am J Surg Pathol. 2015. PMID: 25929349
-
Atypical cribriform lesions of the prostate: relationship to prostatic carcinoma and implication for diagnosis in prostate biopsies.Am J Surg Pathol. 2010 Apr;34(4):470-7. doi: 10.1097/PAS.0b013e3181cfc44b. Am J Surg Pathol. 2010. PMID: 20182345
-
Diagnosis of "Poorly Formed Glands" Gleason Pattern 4 Prostatic Adenocarcinoma on Needle Biopsy: An Interobserver Reproducibility Study Among Urologic Pathologists With Recommendations.Am J Surg Pathol. 2015 Oct;39(10):1331-9. doi: 10.1097/PAS.0000000000000457. Am J Surg Pathol. 2015. PMID: 26099009
-
The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System.Am J Surg Pathol. 2016 Feb;40(2):244-52. doi: 10.1097/PAS.0000000000000530. Am J Surg Pathol. 2016. PMID: 26492179 Review.
-
Clinical significance of subtypes of Gleason pattern 4 prostate cancer.Transl Androl Urol. 2018 Sep;7(Suppl 4):S477-S483. doi: 10.21037/tau.2018.02.06. Transl Androl Urol. 2018. PMID: 30363452 Free PMC article. Review.
Cited by
-
Prostate Pathology: What is New in the 2022 WHO Classification of Urinary and Male Genital Tumors?Pathologica. 2022 Feb;115(1):41-56. doi: 10.32074/1591-951X-822. Epub 2023 Jan 16. Pathologica. 2022. PMID: 36645399 Free PMC article. Review.
-
Cultivating Clinical Clarity through Computer Vision: A Current Perspective on Whole Slide Imaging and Artificial Intelligence.Diagnostics (Basel). 2022 Jul 22;12(8):1778. doi: 10.3390/diagnostics12081778. Diagnostics (Basel). 2022. PMID: 35892487 Free PMC article. Review.
-
WHO Classification of Tumours fifth edition: evolving issues in the classification, diagnosis, and prognostication of prostate cancer.Histopathology. 2022 Oct;81(4):447-458. doi: 10.1111/his.14711. Epub 2022 Aug 2. Histopathology. 2022. PMID: 35758185 Free PMC article. Review.
-
Proposal for an optimised definition of adverse pathology (unfavourable histology) that predicts metastatic risk in prostatic adenocarcinoma independent of grade group and pathological stage.Histopathology. 2024 Oct;85(4):598-613. doi: 10.1111/his.15231. Epub 2024 Jun 3. Histopathology. 2024. PMID: 38828674
-
Analysis of separate training and validation radical prostatectomy cohorts identifies 0.25 mm diameter as an optimal definition for "large" cribriform prostatic adenocarcinoma.Mod Pathol. 2022 Aug;35(8):1092-1100. doi: 10.1038/s41379-022-01009-7. Epub 2022 Feb 10. Mod Pathol. 2022. PMID: 35145197 Free PMC article.
References
-
- Epstein JI, Amin MB, Fine SW, Algaba F, Aron M, Baydar DE, Beltran AL, Brimo F, Cheville JC, Colecchia M, Comperat E, da Cunha IW, Delprado W, DeMarzo AM, Giannico GA, Gordetsky JB, Guo CC, Hansel DE, Hirsch MS, Huang J, Humphrey PA, Jimenez RE, Khani F, Kong Q, Kryvenko ON, Kunju LP, Lal P, Latour M, Lotan T, Maclean F, Magi-Galluzzi C, Mehra R, Menon S, Miyamoto H, Montironi R, Netto GJ, Nguyen JK, Osunkoya AO, Parwani A, Robinson BD, Rubin MA, Shah RB, So JS, Takahashi H, Tavora F, Tretiakova MS, True L, Wobker SE, Yang XJ, Zhou M, Zynger DL, Trpkov K. The 2019 Genitourinary Pathology Society (GUPS) white paper on contemporary grading of prostate cancer. Arch Pathol Lab Med. 2021;145:461–493. - PubMed
-
- Iczkowski KA, Paner GP, Van der Kwast T. The new realization about cribriform prostate cancer. Adv Anat Pathol. 2018;25:31–37. - PubMed
-
- Kweldam CF, Wildhagen MF, Steyerberg EW, Bangma CH, van der Kwast TH, van Leenders GJ. Cribriform growth is highly predictive for postoperative metastasis and disease-specific death in Gleason score 7 prostate cancer. Mod Pathol. 2015;28:457–464. - PubMed
-
- Choy B, Pearce SM, Anderson BB, Shalhav AL, Zagaja G, Eggener SE, Paner GP. Prognostic significance of percentage and architectural types of contemporary gleason pattern 4 prostate cancer in radical prostatectomy. Am J Surg Pathol. 2016;40:1400–1406. - PubMed
LinkOut - more resources
Full Text Sources