

Impact of vitamin D level at diagnosis and transplantation on the prognosis of hematological malignancy: a meta-analysis
- PMID: 34496015
- PMCID: PMC8905698
- DOI: 10.1182/bloodadvances.2021004958
Impact of vitamin D level at diagnosis and transplantation on the prognosis of hematological malignancy: a meta-analysis
Abstract
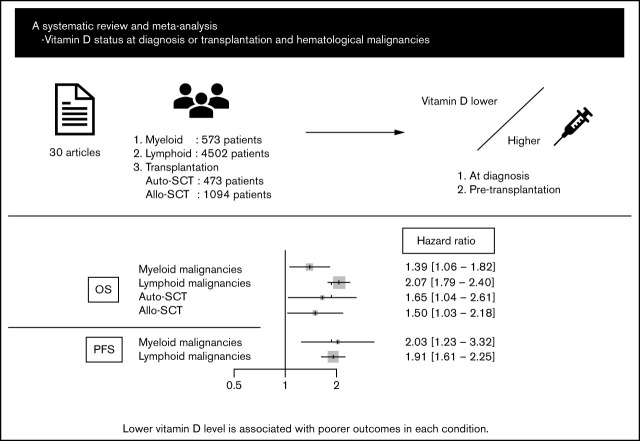
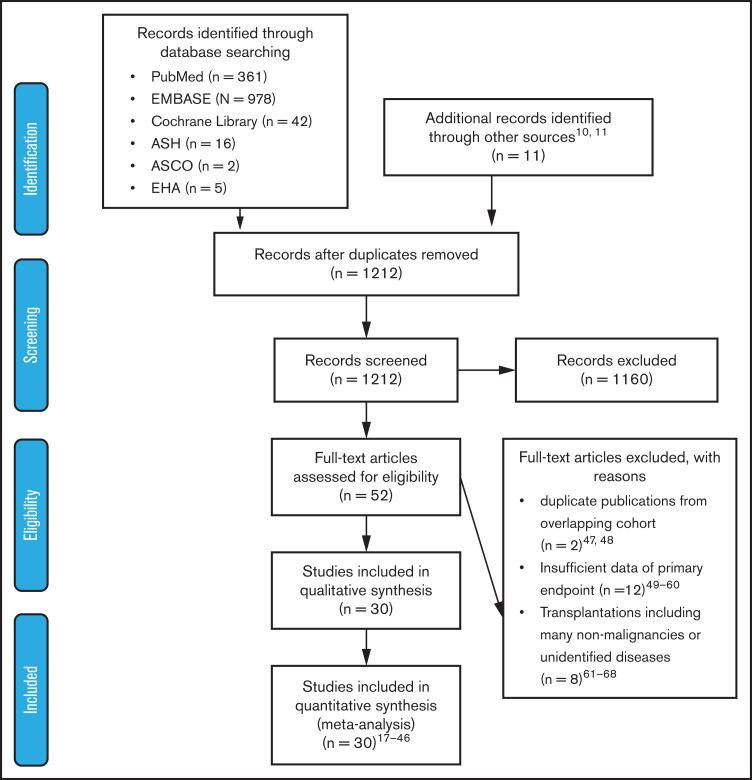
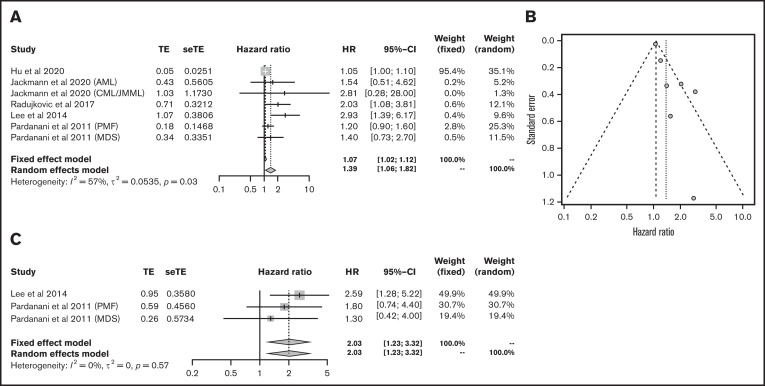
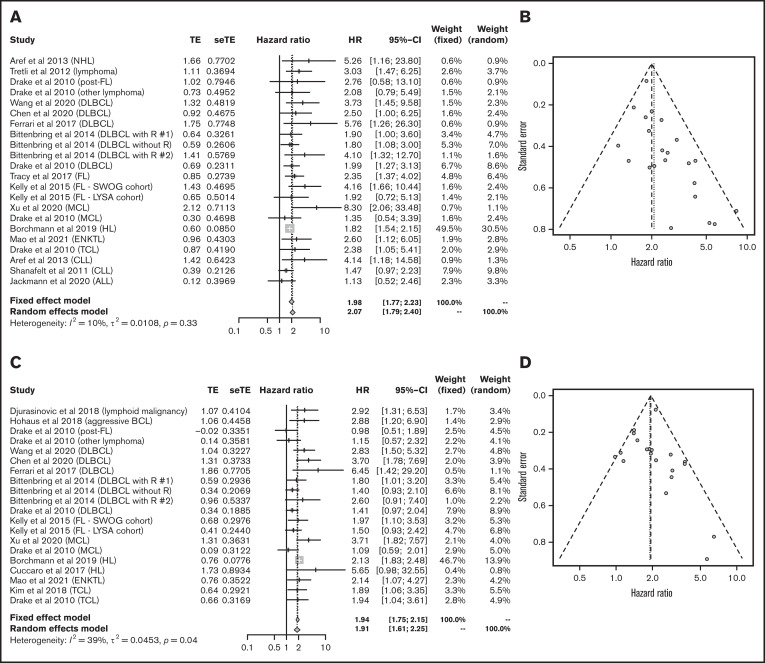
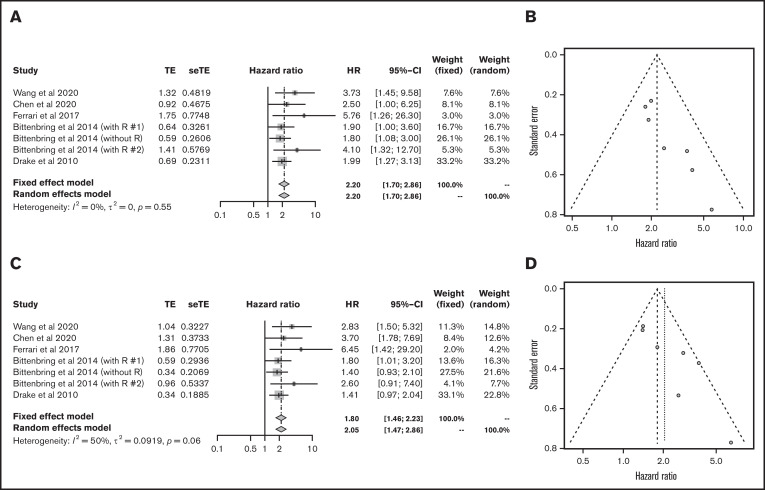
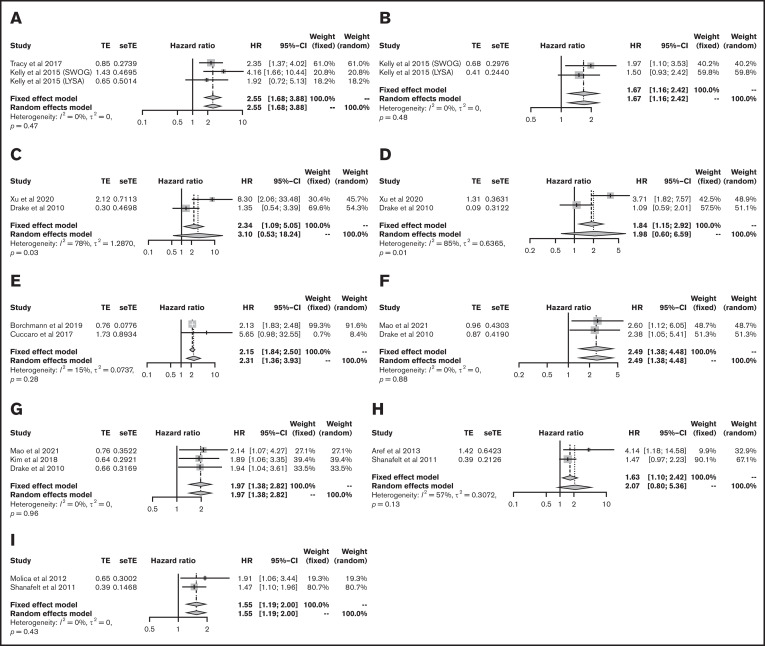
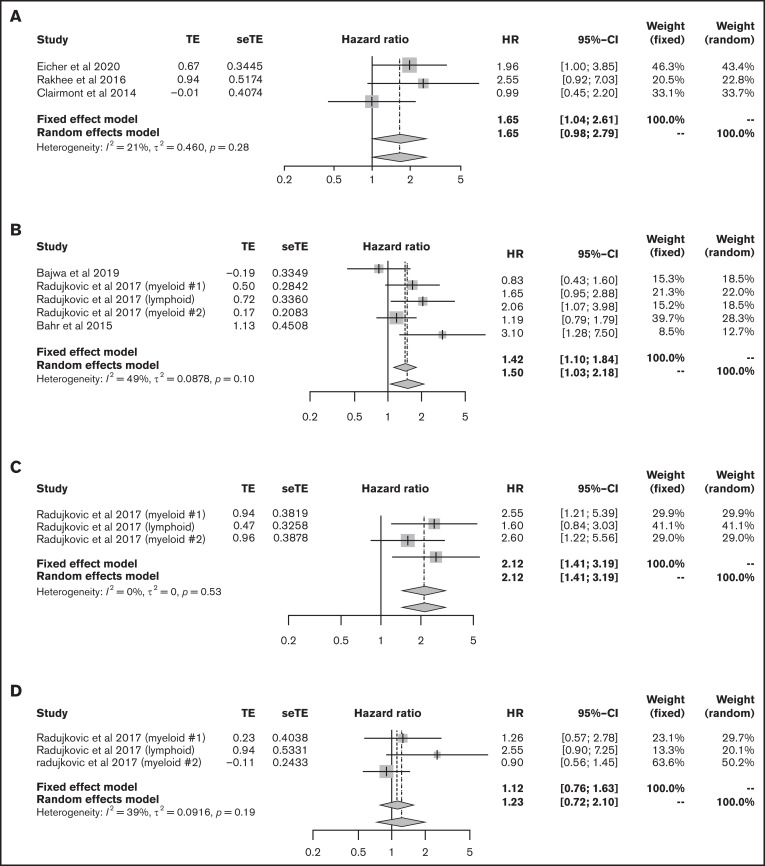
Vitamin D deficiency impairs prognosis in many types of cancer; however, its significance in each subtype of hematological malignancies is unclear. In addition, data on the association between pretransplant vitamin D levels and outcomes of hematopoietic stem cell transplantation (HSCT) are inconsistent. This systematic review and meta-analysis aimed to elucidate the impact of vitamin D levels at diagnosis or pre-HSCT on the prognosis of hematological malignancies. Thirty articles and abstracts were extracted from PubMed, Embase, and Cochrane Library databases and conference proceedings. Fixed and random effect models were used to analyze primary outcomes: overall survival (OS) and progression-free survival (PFS). Lower vitamin D level was significantly associated with poorer OS and PFS in myeloid malignancies (hazard ratio [HR], 1.39; 95% confidence interval [CI], 1.06-1.82 and HR, 2.03; 95% CI, 1.23-3.32, respectively) and lymphoid malignancies (HR, 2.07; 95% CI, 1.79-2.40 and HR, 1.91; 95% CI, 1.61-2.25, respectively), as well as outcomes for several lymphoma subtypes individually. Furthermore, a lower pretransplant vitamin D level was associated with poorer OS in autologous and allogeneic HSCT (HR, 1.65; 95% CI, 1.04-2.61 and HR, 1.50; 95% CI, 1.03-2.18, respectively). Despite the relatively small number of studies evaluated, these data suggest the importance of vitamin D status in outcomes of hematological malignancies (PROSPERO registration number: CRD42020205821).
© 2022 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures
Similar articles
-
Effect of pre-transplantation serum ferritin on outcomes in patients undergoing allogeneic hematopoietic stem cell transplantation: A meta-analysis.Medicine (Baltimore). 2018 Jul;97(27):e10310. doi: 10.1097/MD.0000000000010310. Medicine (Baltimore). 2018. PMID: 29979374 Free PMC article. Review.
-
Serum 25-hydroxyvitamin D levels and prognosis in hematological malignancies: a systematic review and meta-analysis.Cell Physiol Biochem. 2015;35(5):1999-2005. doi: 10.1159/000374007. Epub 2015 Mar 27. Cell Physiol Biochem. 2015. PMID: 25871640 Review.
-
Comparison of Allogeneic Stem Cell Transplant and Autologous Stem Cell Transplant in Refractory or Relapsed Peripheral T-Cell Lymphoma: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 May 3;4(5):e219807. doi: 10.1001/jamanetworkopen.2021.9807. JAMA Netw Open. 2021. PMID: 34042995 Free PMC article.
-
The prognostic impact of the cytomegalovirus serostatus in patients with chronic hematological malignancies after allogeneic hematopoietic stem cell transplantation: a report from the Infectious Diseases Working Party of EBMT.Ann Hematol. 2019 Jul;98(7):1755-1763. doi: 10.1007/s00277-019-03669-z. Epub 2019 Apr 16. Ann Hematol. 2019. PMID: 30993417 Clinical Trial.
-
Allogeneic bone marrow transplantation compared to peripheral blood stem cell transplantation for the treatment of hematologic malignancies: a meta-analysis based on time-to-event data from randomized controlled trials.Ann Hematol. 2012 Mar;91(3):427-37. doi: 10.1007/s00277-011-1299-8. Epub 2011 Jul 26. Ann Hematol. 2012. PMID: 21789620
Cited by
-
Effect of Vitamin D and Skeletal Muscle Mass on Prognosis of Patients with Diffuse Large B-Cell Lymphoma.Nutrients. 2024 Aug 11;16(16):2653. doi: 10.3390/nu16162653. Nutrients. 2024. PMID: 39203790 Free PMC article.
-
Vitamin D and Cancer: An Historical Overview of the Epidemiology and Mechanisms.Nutrients. 2022 Mar 30;14(7):1448. doi: 10.3390/nu14071448. Nutrients. 2022. PMID: 35406059 Free PMC article. Review.
-
Vitamin D deficiency linked to abnormal bone and lipid metabolism predicts high-risk multiple myeloma with poorer prognosis.Front Endocrinol (Lausanne). 2023 Apr 27;14:1157969. doi: 10.3389/fendo.2023.1157969. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37181039 Free PMC article.
-
Awareness on hematological malignancies among college students.J Adv Pharm Technol Res. 2022 Dec;13(Suppl 2):S534-S538. doi: 10.4103/japtr.japtr_175_22. Epub 2022 Dec 30. J Adv Pharm Technol Res. 2022. PMID: 36798560 Free PMC article.
-
The Global Prevalence of Vitamin D Deficiency and Insufficiency in Patients with Multiple Myeloma: A Systematic Review and Meta-Analysis.Nutrients. 2023 Jul 20;15(14):3227. doi: 10.3390/nu15143227. Nutrients. 2023. PMID: 37513645 Free PMC article. Review.
References
-
- Bandera Merchan B, Morcillo S, Martin-Nuñez G, Tinahones FJ, Macías-González M. The role of vitamin D and VDR in carcinogenesis: through epidemiology and basic sciences. J Steroid Biochem Mol Biol. 2017;167:203-218. - PubMed
-
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266-281. - PubMed
-
- Li M, Chen P, Li J, Chu R, Xie D, Wang H. Review: the impacts of circulating 25-hydroxyvitamin D levels on cancer patient outcomes: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99(7):2327-2336. - PubMed
