

Impact of the COVID-19 pandemic in patients with systemic lupus erythematosus throughout one year
- PMID: 34478882
- PMCID: PMC8405598
- DOI: 10.1016/j.clim.2021.108845
Impact of the COVID-19 pandemic in patients with systemic lupus erythematosus throughout one year
Abstract
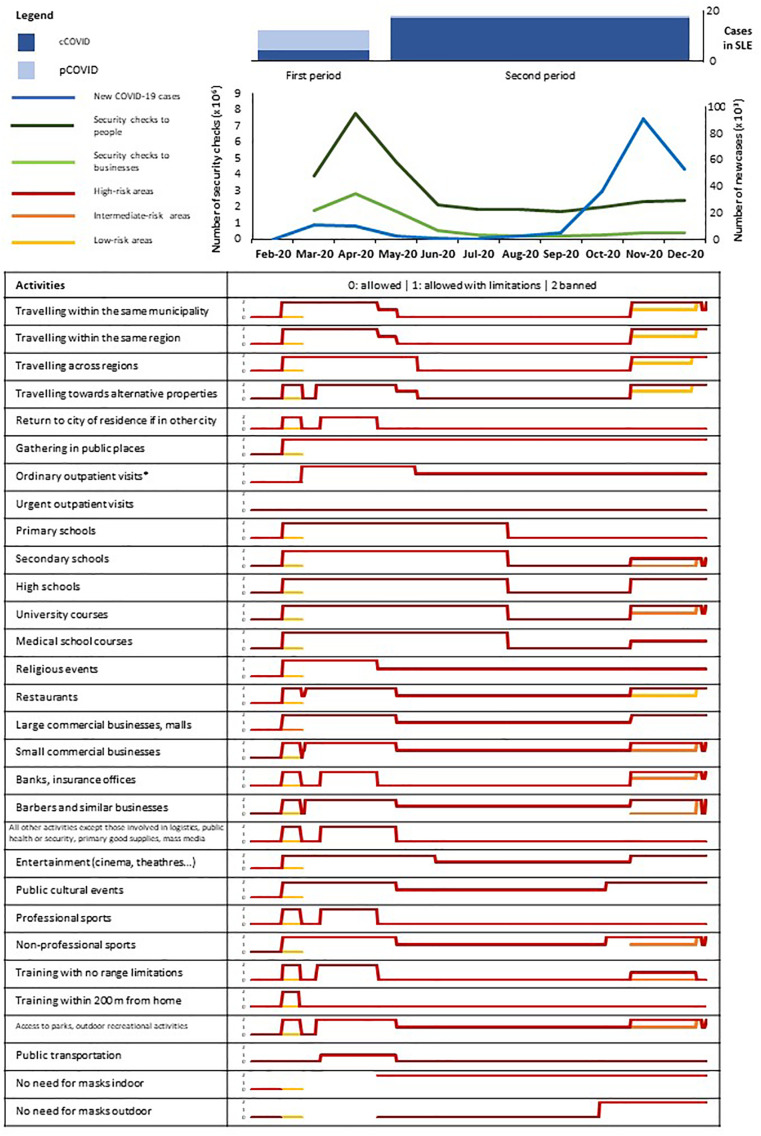
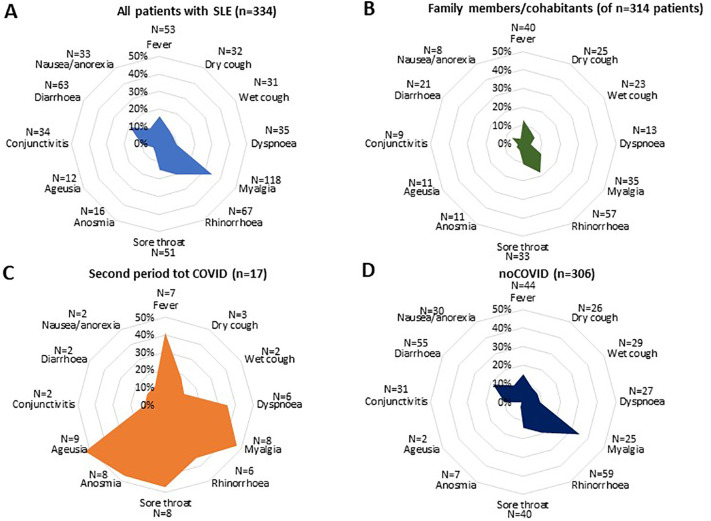
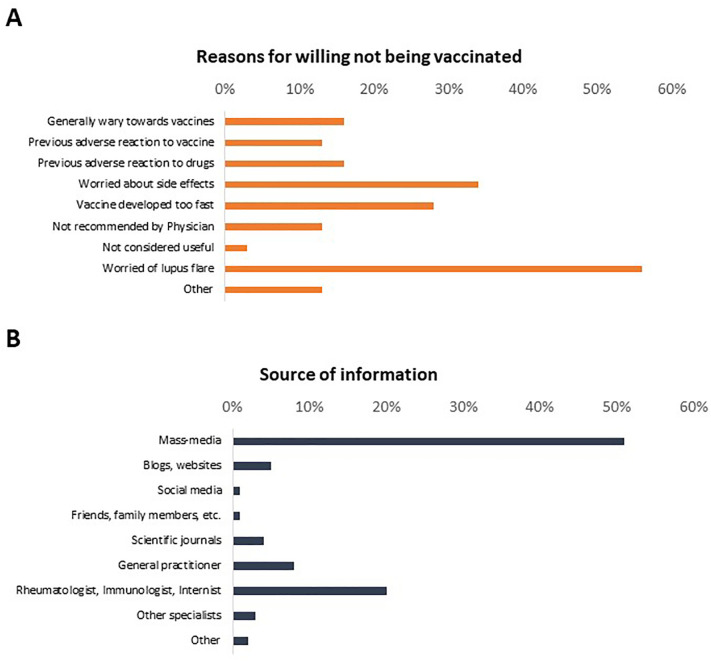
Little is known about the impact of coronavirus disease 2019 (COVID-19) pandemic to the care of patients with systemic lupus erythematosus (SLE) in the long-term. By crossing population data with the results of a web-based survey focused on the timeframes January-April and May-December 2020, we found that among 334/518 responders, 28 had COVID-19 in 2020. Seventeen cases occurred in May-December, in parallel with trends in the general population and loosening of containment policy strength. Age > 40 years (p = 0.026), prednisone escalation (p = 0.008) and infected relatives (p < 0.001) were most significantly associated with COVID-19. Weaker associations were found with asthma, lymphadenopathy and azathioprine or cyclosporine treatment. Only 31% of patients with infected relatives developed COVID-19. Healthcare service disruptions were not associated with rising hospitalisations. Vaccination prospects were generally welcomed. Our data suggest that COVID-19 has a moderate impact on patients with SLE, which might be significantly modulated by public health policies, including vaccination.
Keywords: COVID-19; Containment; Coronavirus; Lockdown; Prednisone; Public health; Systemic lupus erythematosus; Treatment; Vaccination.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Evaluation of Immune Response and Disease Status in Systemic Lupus Erythematosus Patients Following SARS-CoV-2 Vaccination.Arthritis Rheumatol. 2022 Feb;74(2):284-294. doi: 10.1002/art.41937. Epub 2021 Dec 28. Arthritis Rheumatol. 2022. PMID: 34347939 Free PMC article.
-
Cyclosporine may reduce the risk of symptomatic COVID-19 in patients with systemic lupus erythematosus: a retrospective cohort study.Microbiol Spectr. 2024 Nov 5;12(11):e0127624. doi: 10.1128/spectrum.01276-24. Epub 2024 Oct 15. Microbiol Spectr. 2024. PMID: 39404351 Free PMC article.
-
Systemic Lupus Erythematosus and COVID-19.Curr Rheumatol Rep. 2023 Oct;25(10):192-203. doi: 10.1007/s11926-023-01110-z. Epub 2023 Jul 21. Curr Rheumatol Rep. 2023. PMID: 37477841 Free PMC article. Review.
-
SARS-CoV-2 Antibody Isotypes in Systemic Lupus Erythematosus Patients Prior to Vaccination: Associations With Disease Activity, Antinuclear Antibodies, and Immunomodulatory Drugs During the First Year of the Pandemic.Front Immunol. 2021 Aug 27;12:724047. doi: 10.3389/fimmu.2021.724047. eCollection 2021. Front Immunol. 2021. PMID: 34512651 Free PMC article.
-
Lupus, vaccinations and COVID-19: What we know now.Lupus. 2021 Sep;30(10):1541-1552. doi: 10.1177/09612033211024355. Epub 2021 Jun 17. Lupus. 2021. PMID: 34134555 Review.
Cited by
-
Efficacy and Safety of Anti-SARS-CoV-2 Antiviral Agents and Monoclonal Antibodies in Patients with SLE: A Case-Control Study.Biomolecules. 2023 Aug 22;13(9):1273. doi: 10.3390/biom13091273. Biomolecules. 2023. PMID: 37759674 Free PMC article.
-
Medium-term impact of the SARS-CoV-2 mRNA vaccine against disease activity in patients with systemic lupus erythematosus.Lupus Sci Med. 2022 Aug;9(1):e000727. doi: 10.1136/lupus-2022-000727. Lupus Sci Med. 2022. PMID: 35961691 Free PMC article.
-
Impact of COVID-19 pandemic on healthcare provision in youth with systemic lupus erythematosus.Clin Exp Pediatr. 2024 Nov;67(11):628-631. doi: 10.3345/cep.2024.00689. Epub 2024 Oct 28. Clin Exp Pediatr. 2024. PMID: 39463337 Free PMC article. No abstract available.
-
Breakthrough SARS-CoV-2 infection in fully vaccinated patients with systemic lupus erythematosus: results from the COVID-19 Vaccination in Autoimmune Disease (COVAD) study.Rheumatol Int. 2024 Oct;44(10):1923-1933. doi: 10.1007/s00296-024-05682-6. Epub 2024 Aug 13. Rheumatol Int. 2024. PMID: 39138675 Free PMC article.
-
Cardiac Safety of mRNA-Based Vaccines in Patients with Systemic Lupus Erythematosus and Lupus-like Disorders with a History of Myocarditis.Pathogens. 2022 Sep 1;11(9):1001. doi: 10.3390/pathogens11091001. Pathogens. 2022. PMID: 36145434 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
