

Distinct time courses and mechanics of right ventricular hypertrophy and diastolic stiffening in a male rat model of pulmonary arterial hypertension
- PMID: 34448637
- PMCID: PMC8794227
- DOI: 10.1152/ajpheart.00046.2021
Distinct time courses and mechanics of right ventricular hypertrophy and diastolic stiffening in a male rat model of pulmonary arterial hypertension
Abstract
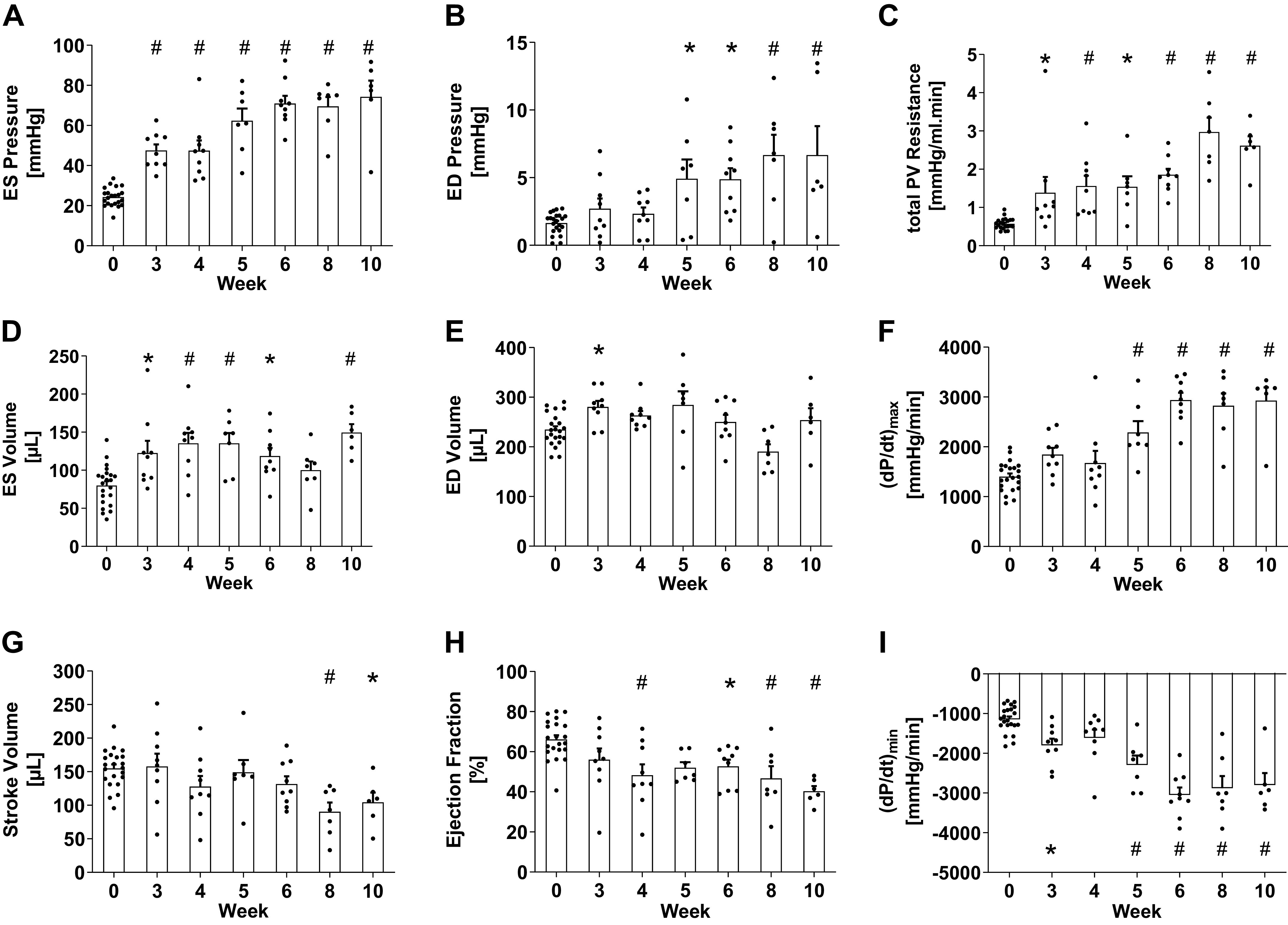
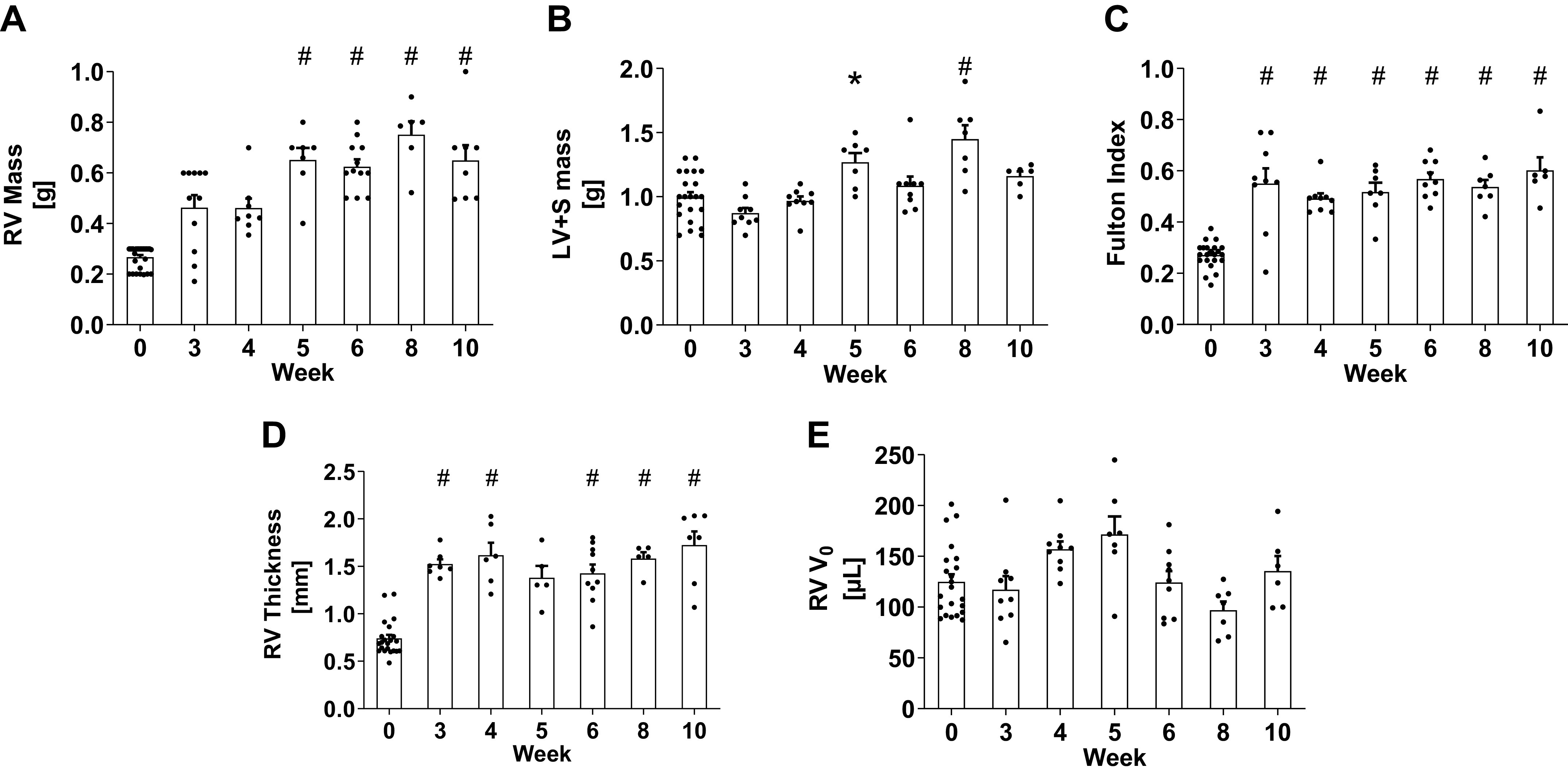
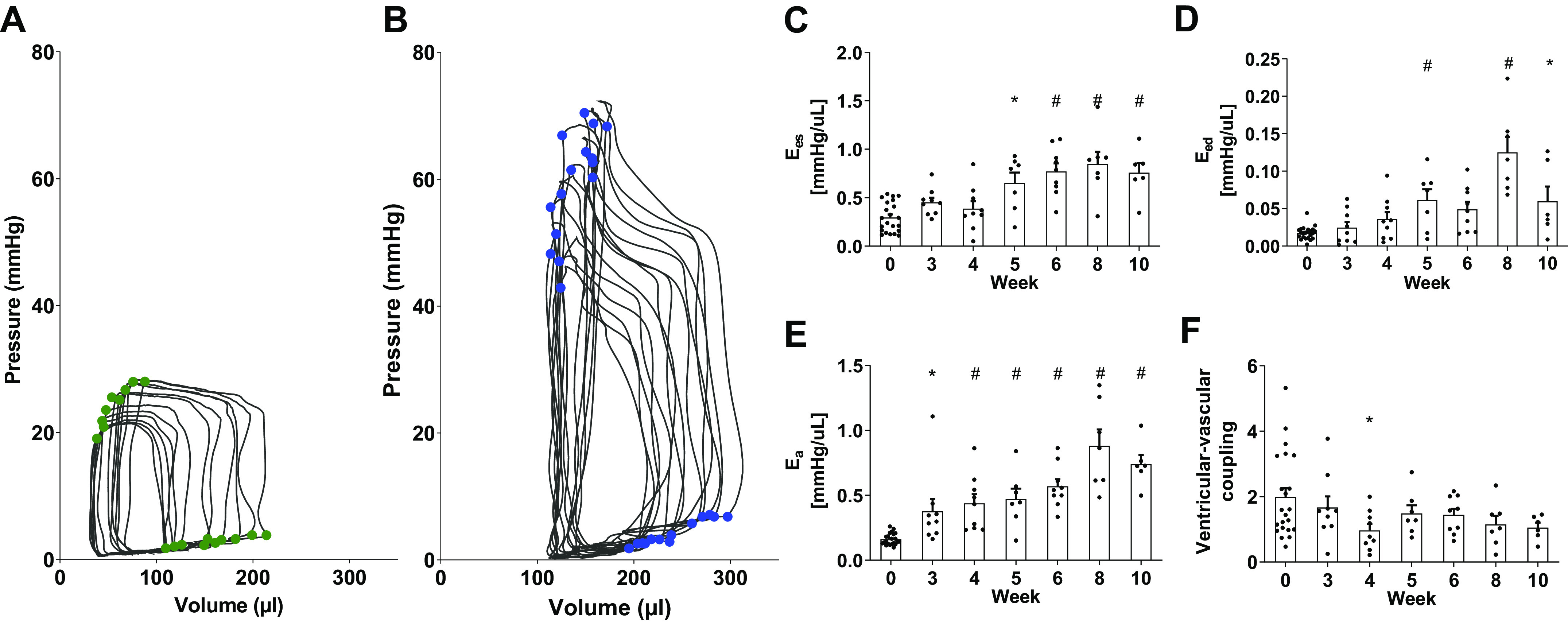
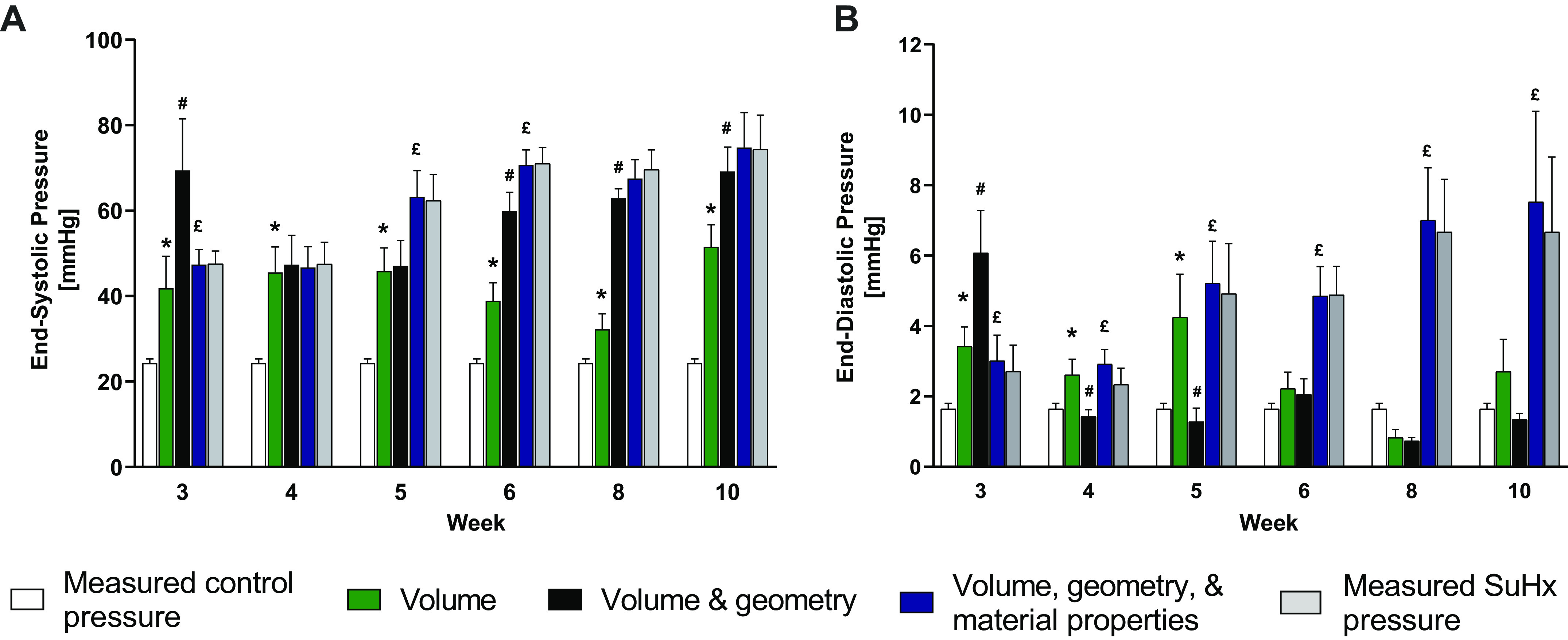
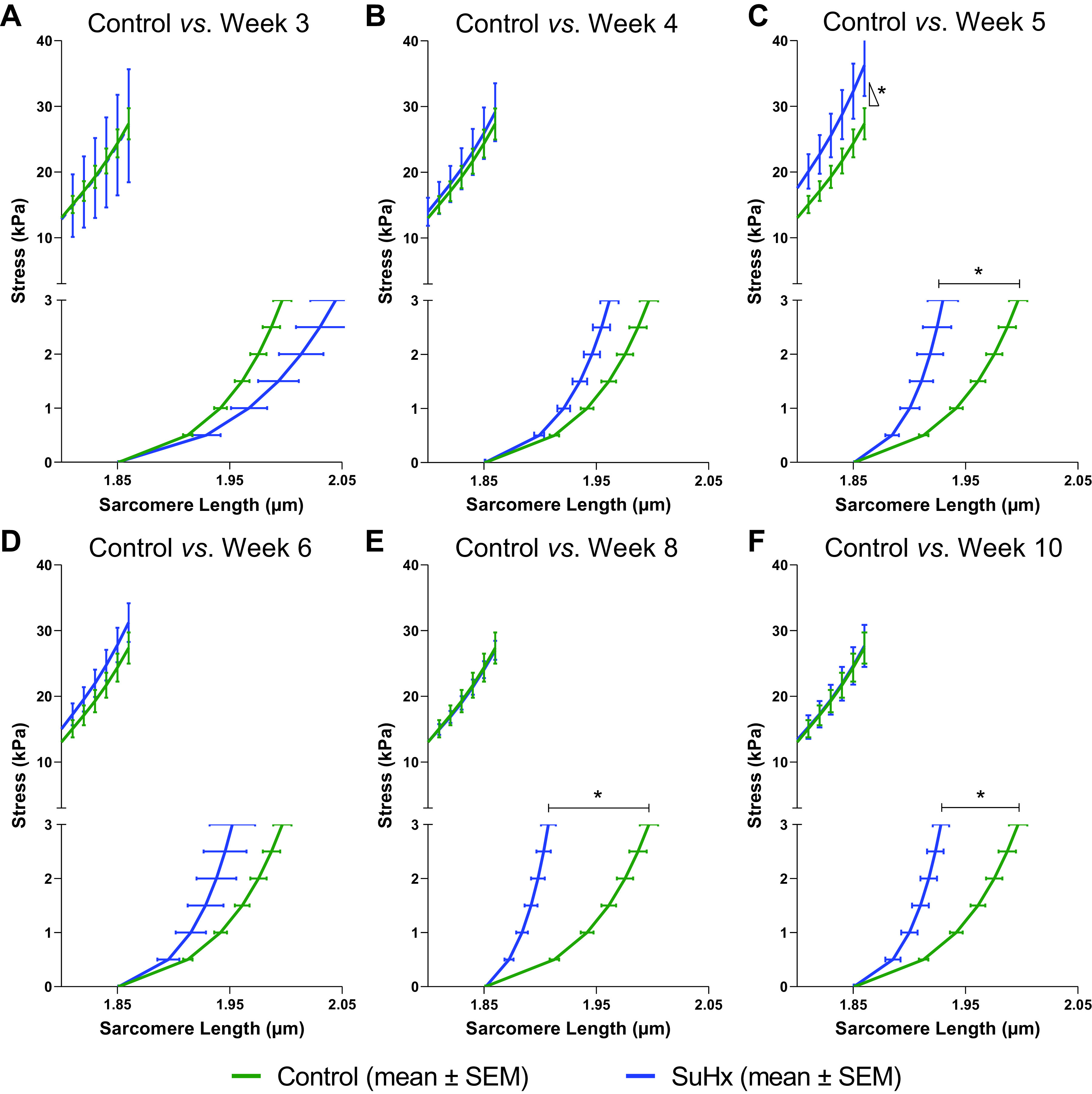
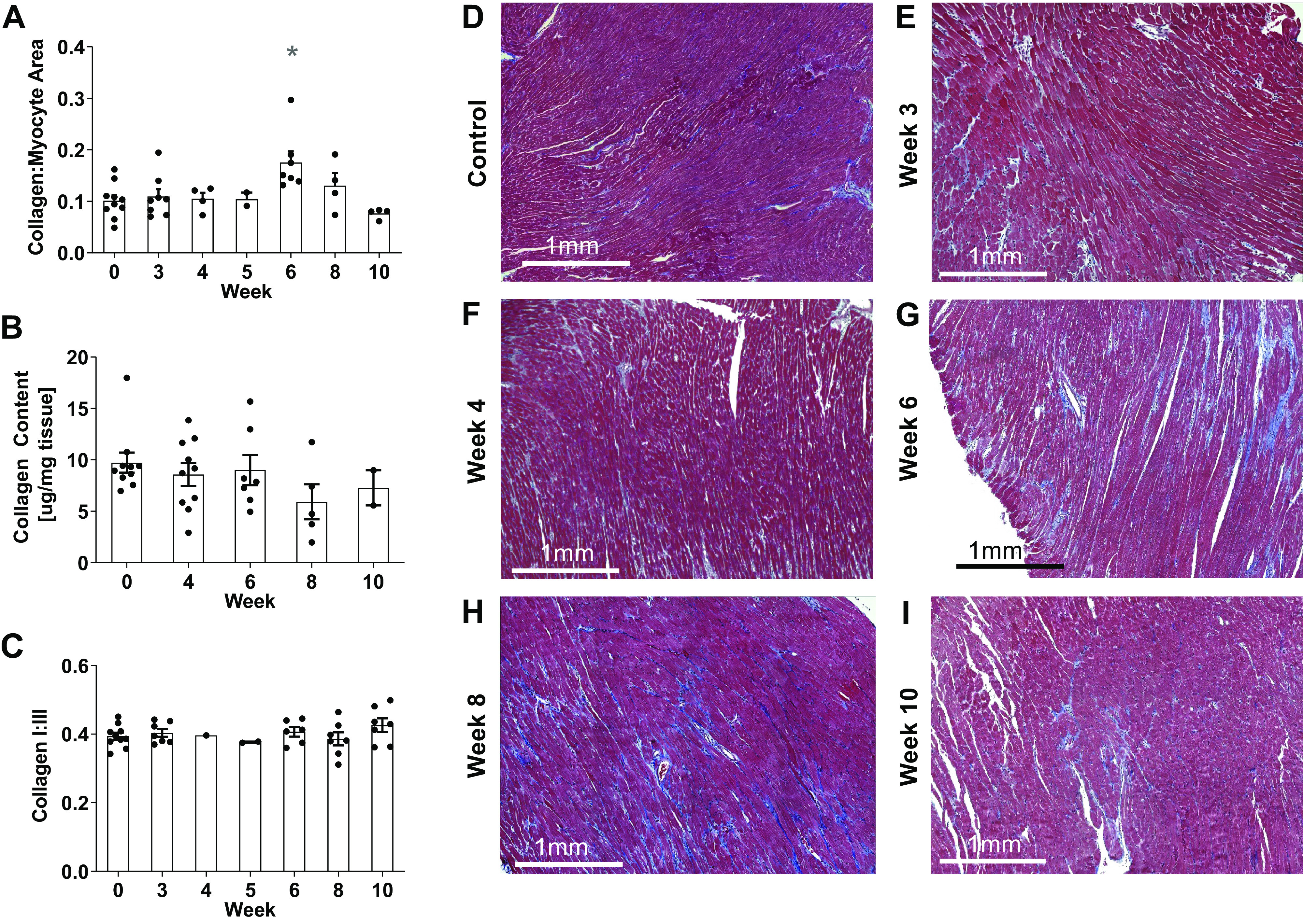
Although pulmonary arterial hypertension (PAH) leads to right ventricle (RV) hypertrophy and structural remodeling, the relative contributions of changes in myocardial geometric and mechanical properties to systolic and diastolic chamber dysfunction and their time courses remain unknown. Using measurements of RV hemodynamic and morphological changes over 10 wk in a male rat model of PAH and a mathematical model of RV mechanics, we discriminated the contributions of RV geometric remodeling and alterations of myocardial material properties to changes in systolic and diastolic chamber function. Significant and rapid RV hypertrophic wall thickening was sufficient to stabilize ejection fraction in response to increased pulmonary arterial pressure by week 4 without significant changes in systolic myofilament activation. After week 4, RV end-diastolic pressure increased significantly with no corresponding changes in end-diastolic volume. Significant RV diastolic chamber stiffening by week 5 was not explained by RV hypertrophy. Instead, model analysis showed that the increases in RV end-diastolic chamber stiffness were entirely attributable to increased resting myocardial material stiffness that was not associated with significant myocardial fibrosis or changes in myocardial collagen content or type. These findings suggest that whereas systolic volume in this model of RV pressure overload is stabilized by early RV hypertrophy, diastolic dilation is prevented by subsequent resting myocardial stiffening.NEW & NOTEWORTHY Using a novel combination of hemodynamic and morphological measurements over 10 wk in a male rat model of PAH and a mathematical model of RV mechanics, we found that compensated systolic function was almost entirely explained by RV hypertrophy, but subsequently altered RV end-diastolic mechanics were primarily explained by passive myocardial stiffening that was not associated with significant collagen extracellular matrix accumulation.
Keywords: diastolic function; mathematical modeling; pulmonary arterial hypertension; sugen-hypoxia; systolic function.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
Similar articles
-
Sex-dependent remodeling of right ventricular function in a rat model of pulmonary arterial hypertension.Am J Physiol Heart Circ Physiol. 2024 Aug 1;327(2):H351-H363. doi: 10.1152/ajpheart.00098.2024. Epub 2024 Jun 7. Am J Physiol Heart Circ Physiol. 2024. PMID: 38847755
-
Impact of Right Ventricular Pressure Overload on Myocardial Stiffness Assessed by Natural Wave Imaging.JACC Cardiovasc Imaging. 2025 Feb;18(2):211-225. doi: 10.1016/j.jcmg.2024.06.020. Epub 2024 Aug 21. JACC Cardiovasc Imaging. 2025. PMID: 39177563
-
Severity of structural and functional right ventricular remodeling depends on training load in an experimental model of endurance exercise.Am J Physiol Heart Circ Physiol. 2017 Sep 1;313(3):H459-H468. doi: 10.1152/ajpheart.00763.2016. Epub 2017 May 26. Am J Physiol Heart Circ Physiol. 2017. PMID: 28550178
-
Excitation-contraction coupling and relaxation alteration in right ventricular remodelling caused by pulmonary arterial hypertension.Arch Cardiovasc Dis. 2020 Jan;113(1):70-84. doi: 10.1016/j.acvd.2019.10.009. Epub 2020 Jan 8. Arch Cardiovasc Dis. 2020. PMID: 31924541 Review.
-
RV pressure overload: from hypertrophy to failure.Cardiovasc Res. 2017 Oct 1;113(12):1423-1432. doi: 10.1093/cvr/cvx145. Cardiovasc Res. 2017. PMID: 28957530 Review.
Cited by
-
Characterizing the Spatiotemporal Transcriptomic Response of the Right Ventricle to Acute Pressure Overload.Int J Mol Sci. 2023 Jun 5;24(11):9746. doi: 10.3390/ijms24119746. Int J Mol Sci. 2023. PMID: 37298696 Free PMC article.
-
A computational study of right ventricular mechanics in a rat model of pulmonary arterial hypertension.Front Physiol. 2024 Mar 11;15:1360389. doi: 10.3389/fphys.2024.1360389. eCollection 2024. Front Physiol. 2024. PMID: 38529483 Free PMC article.
-
Dissecting contributions of pulmonary arterial remodeling to right ventricular afterload in pulmonary hypertension.bioRxiv [Preprint]. 2024 Aug 19:2024.08.18.608471. doi: 10.1101/2024.08.18.608471. bioRxiv. 2024. PMID: 39229168 Free PMC article. Preprint.
-
Right ventricular diastolic adaptation to pressure overload in different rat strains.Physiol Rep. 2024 Jul;12(13):e16132. doi: 10.14814/phy2.16132. Physiol Rep. 2024. PMID: 38993022 Free PMC article.
-
Untangling the mechanisms of pulmonary hypertension-induced right ventricular stiffening in a large animal model.bioRxiv [Preprint]. 2023 Apr 6:2023.04.03.535491. doi: 10.1101/2023.04.03.535491. bioRxiv. 2023. Update in: Acta Biomater. 2023 Nov;171:155-165. doi: 10.1016/j.actbio.2023.09.043. PMID: 37066294 Free PMC article. Updated. Preprint.
References
-
- Rain S, Handoko ML, Trip P, Gan CTJ, Westerhof N, Stienen GJ, Paulus WJ, Ottenheijm CAC, Marcus JT, Dorfmüller P, Guignabert C, Humbert M, Macdonald P, Dos Remedios C, Postmus PE, Saripalli C, Hidalgo CG, Granzier HL, Vonk-Noordegraaf A, Van Der Velden J, De Man FS. Right ventricular diastolic impairment in patients with pulmonary arterial hypertension. Circulation 128: 2016–2025, 2013. doi:10.1161/CIRCULATIONAHA.113.001873. - DOI - PubMed
-
- Gan CT-J, Holverda S, Marcus JT, Paulus WJ, Marques KM, Bronzwaer JGF, Twisk JW, Boonstra A, Postmus PE, Vonk-Noordegraaf A. Right ventricular diastolic dysfunction and the acute effects of sildenafil in pulmonary hypertension patients. Chest 132: 11–17, 2007. doi:10.1378/chest.06-1263. - DOI - PubMed
-
- Swift AJ, Capener D, Johns C, Hamilton N, Rothman A, Elliot C, Condliffe R, Charalampopoulos A, Rajaram S, Lawrie A, Campbell MJ, Wild JM, Kiely DG. Magnetic resonance imaging in the prognostic evaluation of patients with pulmonary arterial hypertension. Am J Respir Crit Care Med 196: 228–239, 2017. doi:10.1164/rccm.201611-2365OC. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources