

Transient Depletion of Foxp3+ Regulatory T Cells Selectively Promotes Aggressive β Cell Autoimmunity in Genetically Susceptible DEREG Mice
- PMID: 34447385
- PMCID: PMC8382961
- DOI: 10.3389/fimmu.2021.720133
Transient Depletion of Foxp3+ Regulatory T Cells Selectively Promotes Aggressive β Cell Autoimmunity in Genetically Susceptible DEREG Mice
Abstract
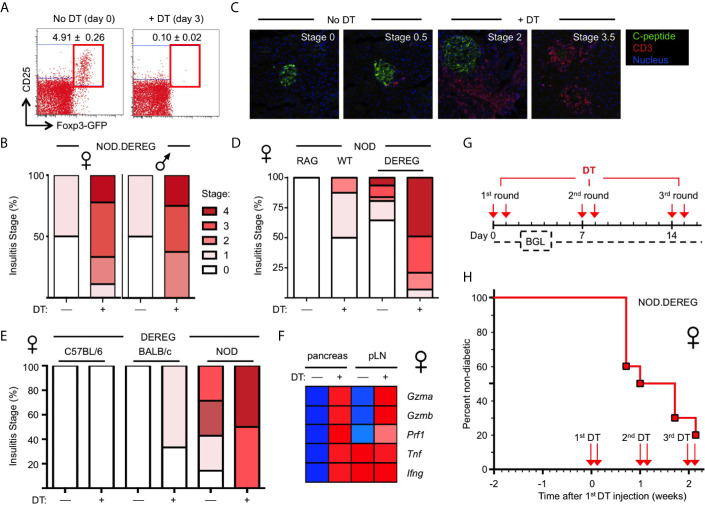
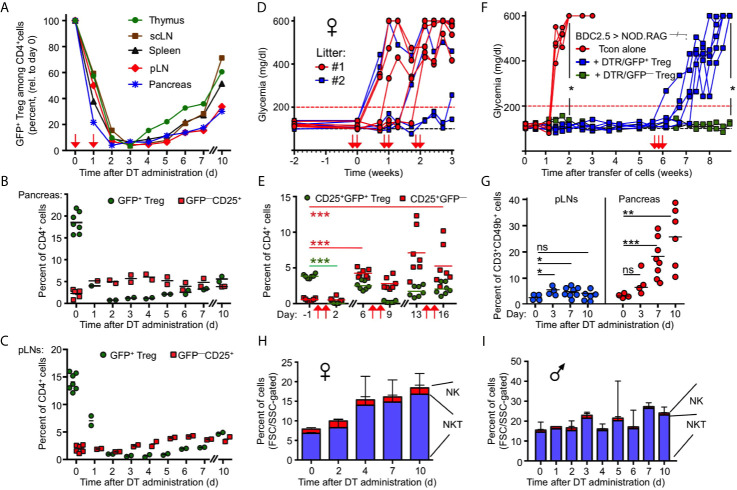
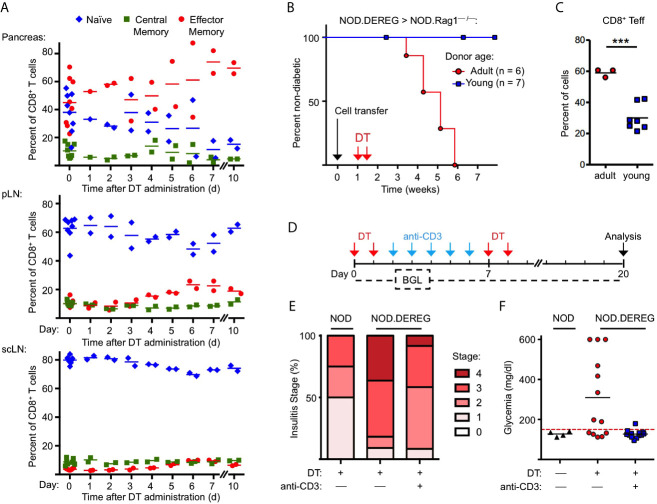
Type 1 diabetes (T1D) represents a hallmark of the fatal multiorgan autoimmune syndrome affecting humans with abrogated Foxp3+ regulatory T (Treg) cell function due to Foxp3 gene mutations, but whether the loss of Foxp3+ Treg cell activity is indeed sufficient to promote β cell autoimmunity requires further scrutiny. As opposed to human Treg cell deficiency, β cell autoimmunity has not been observed in non-autoimmune-prone mice with constitutive Foxp3 deficiency or after diphtheria toxin receptor (DTR)-mediated ablation of Foxp3+ Treg cells. In the spontaneous nonobese diabetic (NOD) mouse model of T1D, constitutive Foxp3 deficiency did not result in invasive insulitis and hyperglycemia, and previous studies on Foxp3+ Treg cell ablation focused on Foxp3DTR NOD mice, in which expression of a transgenic BDC2.5 T cell receptor (TCR) restricted the CD4+ TCR repertoire to a single diabetogenic specificity. Here we revisited the effect of acute Foxp3+ Treg cell ablation on β cell autoimmunity in NOD mice in the context of a polyclonal TCR repertoire. For this, we took advantage of the well-established DTR/GFP transgene of DEREG mice, which allows for specific ablation of Foxp3+ Treg cells without promoting catastrophic autoimmune diseases. We show that the transient loss of Foxp3+ Treg cells in prediabetic NOD.DEREG mice is sufficient to precipitate severe insulitis and persistent hyperglycemia within 5 days after DT administration. Importantly, DT-treated NOD.DEREG mice preserved many clinical features of spontaneous diabetes progression in the NOD model, including a prominent role of diabetogenic CD8+ T cells in terminal β cell destruction. Despite the severity of destructive β cell autoimmunity, anti-CD3 mAb therapy of DT-treated mice interfered with the progression to overt diabetes, indicating that the novel NOD.DEREG model can be exploited for preclinical studies on T1D under experimental conditions of synchronized, advanced β cell autoimmunity. Overall, our studies highlight the continuous requirement of Foxp3+ Treg cell activity for the control of genetically pre-installed autoimmune diabetes.
Keywords: Foxp3; Treg cells; cell ablation; immune regulation; type 1 diabetes.
Copyright © 2021 Watts, Janßen, Jaykar, Palmucci, Weigelt, Petzold, Hommel, Sparwasser, Bonifacio and Kretschmer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Self-Transducible Bimodal PDX1-FOXP3 Protein Lifts Insulin Secretion and Curbs Autoimmunity, Boosting Tregs in Type 1 Diabetic Mice.Mol Ther. 2018 Jan 3;26(1):184-198. doi: 10.1016/j.ymthe.2017.08.014. Epub 2017 Sep 7. Mol Ther. 2018. PMID: 28988715 Free PMC article.
-
Th1-Like ICOS+ Foxp3+ Treg Cells Preferentially Express CXCR3 and Home to β-Islets during Pre-Diabetes in BDC2.5 NOD Mice.PLoS One. 2015 May 6;10(5):e0126311. doi: 10.1371/journal.pone.0126311. eCollection 2015. PLoS One. 2015. PMID: 25946021 Free PMC article.
-
Few Foxp3⁺ regulatory T cells are sufficient to protect adult mice from lethal autoimmunity.Eur J Immunol. 2014 Oct;44(10):2990-3002. doi: 10.1002/eji.201344315. Epub 2014 Aug 11. Eur J Immunol. 2014. PMID: 25042334
-
Control of type 1 autoimmune diabetes by naturally occurring CD4+CD25+ regulatory T lymphocytes in neonatal NOD mice.Ann N Y Acad Sci. 2005 Jun;1051:72-87. doi: 10.1196/annals.1361.048. Ann N Y Acad Sci. 2005. PMID: 16126946 Review.
-
The importance of the Non Obese Diabetic (NOD) mouse model in autoimmune diabetes.J Autoimmun. 2016 Jan;66:76-88. doi: 10.1016/j.jaut.2015.08.019. Epub 2015 Sep 26. J Autoimmun. 2016. PMID: 26403950 Free PMC article. Review.
Cited by
-
Intestinal flora: a potential pathogenesis mechanism and treatment strategy for type 1 diabetes mellitus.Gut Microbes. 2024 Jan-Dec;16(1):2423024. doi: 10.1080/19490976.2024.2423024. Epub 2024 Nov 9. Gut Microbes. 2024. PMID: 39520706 Free PMC article. Review.
-
The amphiregulin/EGFR axis has limited contribution in controlling autoimmune diabetes.Sci Rep. 2023 Oct 30;13(1):18653. doi: 10.1038/s41598-023-45738-4. Sci Rep. 2023. PMID: 37903947 Free PMC article.
-
Epigenetic regulation and T-cell responses in endometriosis - something other than autoimmunity.Front Immunol. 2022 Jul 22;13:943839. doi: 10.3389/fimmu.2022.943839. eCollection 2022. Front Immunol. 2022. PMID: 35935991 Free PMC article. Review.
-
Exenatide regulates Th17/Treg balance via PI3K/Akt/FoxO1 pathway in db/db mice.Mol Med. 2022 Dec 3;28(1):144. doi: 10.1186/s10020-022-00574-6. Mol Med. 2022. PMID: 36463128 Free PMC article.
-
Selective ablation of thymic and peripheral Foxp3+ regulatory T cell development.Front Immunol. 2023 Dec 18;14:1298938. doi: 10.3389/fimmu.2023.1298938. eCollection 2023. Front Immunol. 2023. PMID: 38164128 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials