

BET bromodomain protein inhibition reverses chimeric antigen receptor extinction and reinvigorates exhausted T cells in chronic lymphocytic leukemia
- PMID: 34396987
- PMCID: PMC8363276
- DOI: 10.1172/JCI145459
BET bromodomain protein inhibition reverses chimeric antigen receptor extinction and reinvigorates exhausted T cells in chronic lymphocytic leukemia
Abstract
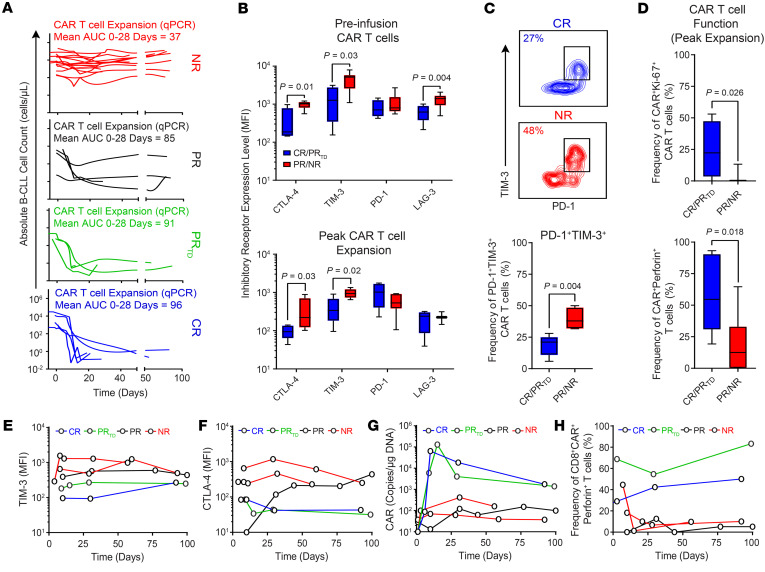
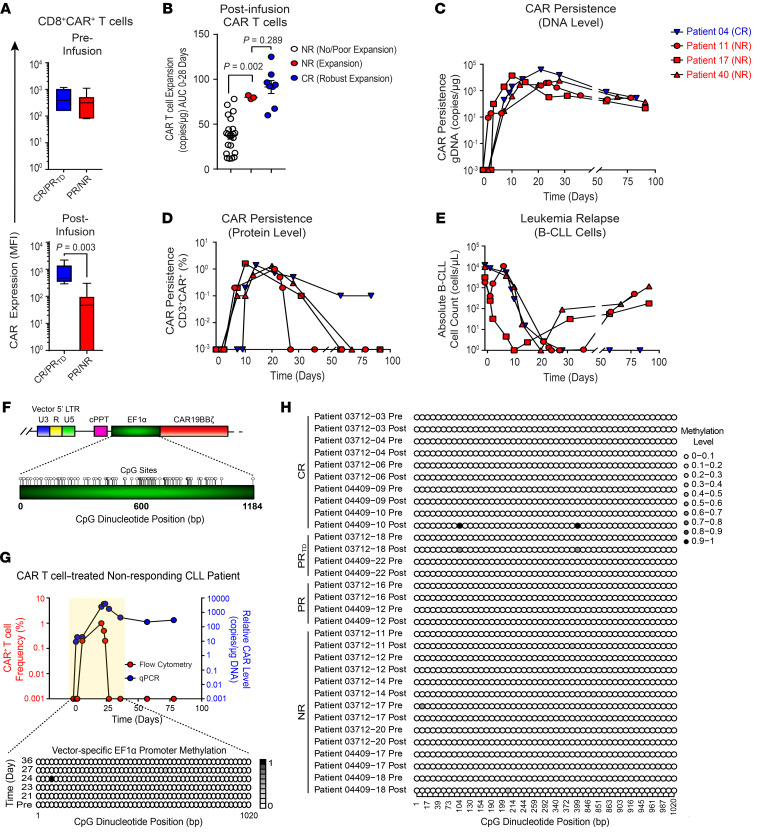
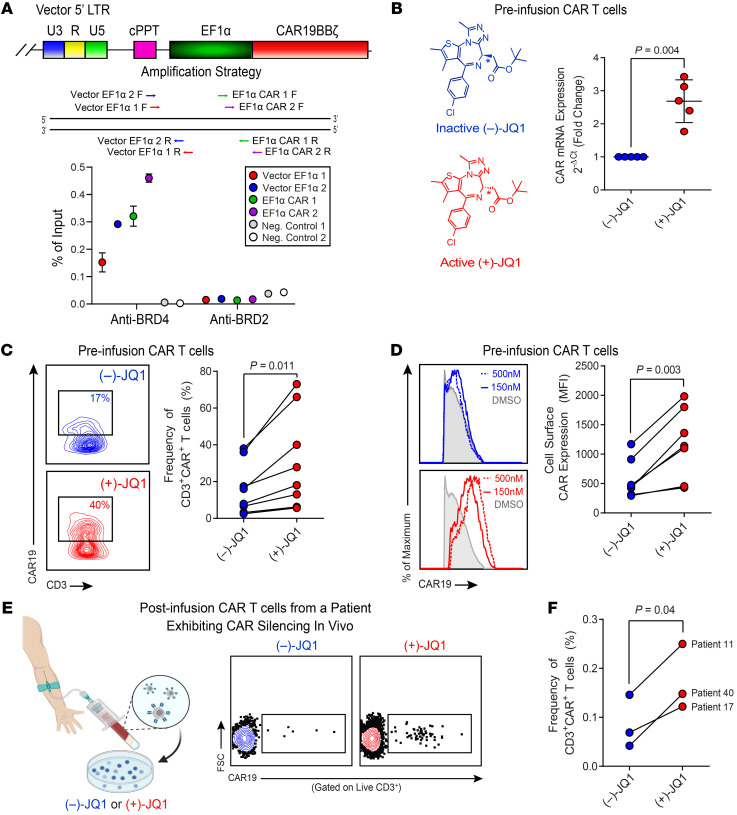
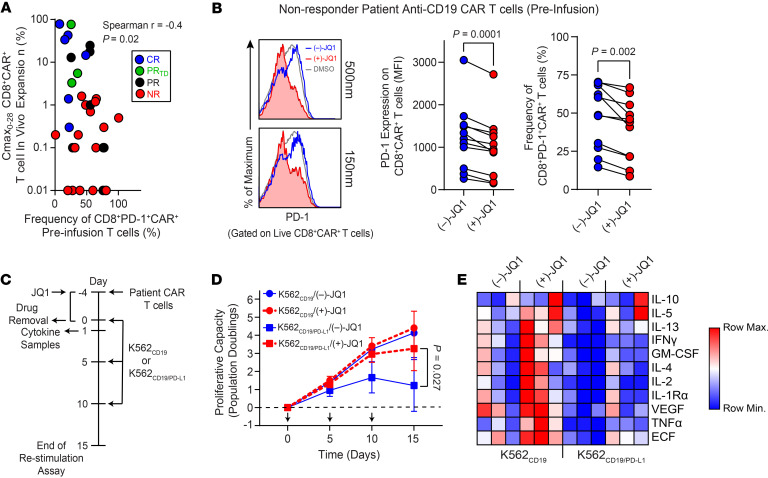
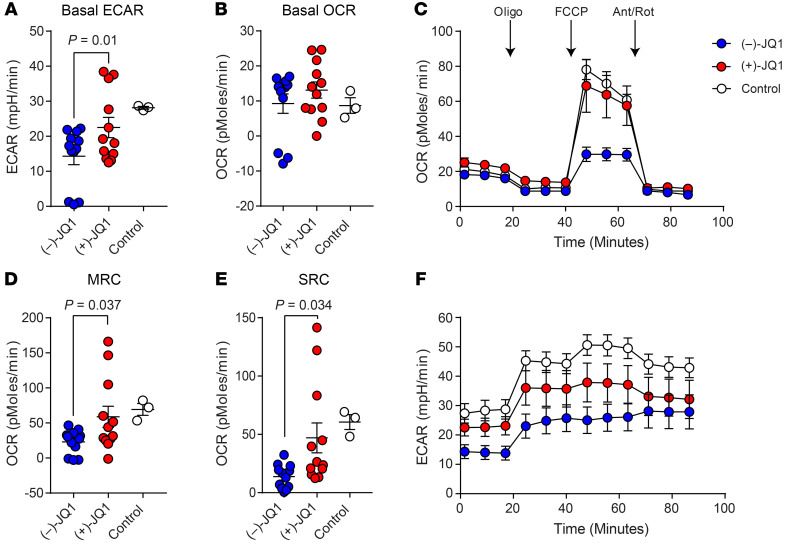
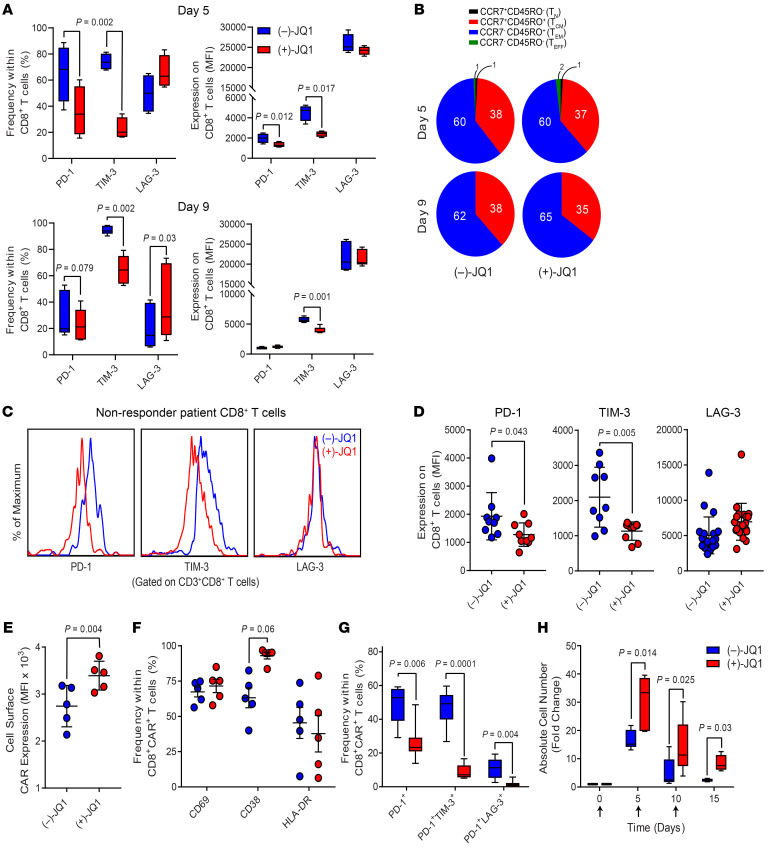
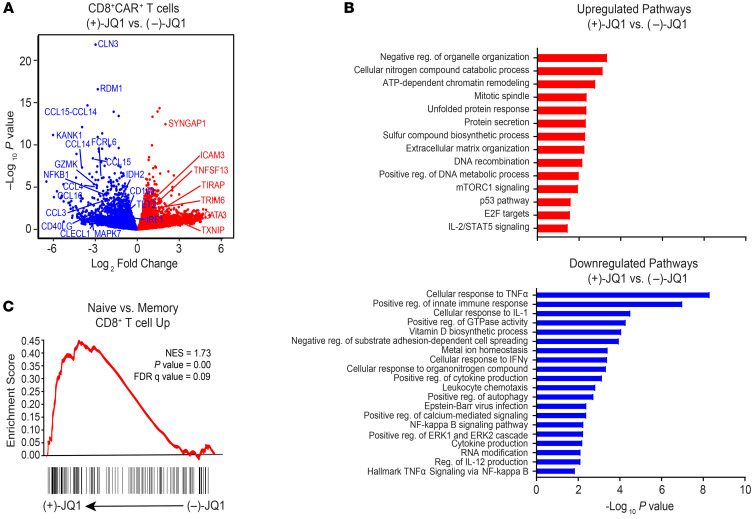
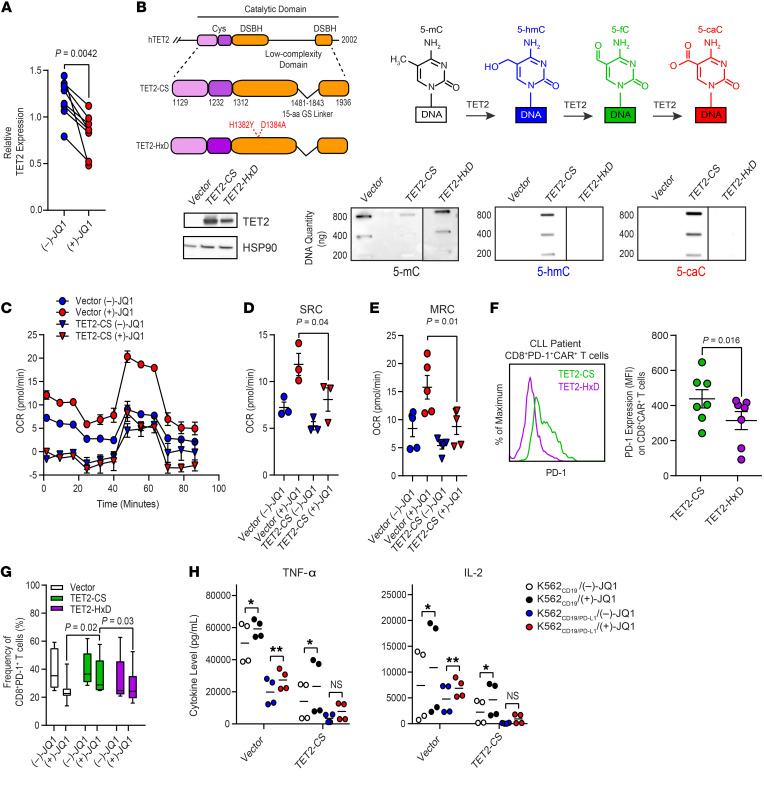
Chimeric antigen receptor (CAR) T cells have induced remarkable antitumor responses in B cell malignancies. Some patients do not respond because of T cell deficiencies that hamper the expansion, persistence, and effector function of these cells. We used longitudinal immune profiling to identify phenotypic and pharmacodynamic changes in CD19-directed CAR T cells in patients with chronic lymphocytic leukemia (CLL). CAR expression maintenance was also investigated because this can affect response durability. CAR T cell failure was accompanied by preexisting T cell-intrinsic defects or dysfunction acquired after infusion. In a small subset of patients, CAR silencing was observed coincident with leukemia relapse. Using a small molecule inhibitor, we demonstrated that the bromodomain and extra-terminal (BET) family of chromatin adapters plays a role in downregulating CAR expression. BET protein blockade also ameliorated CAR T cell exhaustion as manifested by inhibitory receptor reduction, enhanced metabolic fitness, increased proliferative capacity, and enriched transcriptomic signatures of T cell reinvigoration. BET inhibition decreased levels of the TET2 methylcytosine dioxygenase, and forced expression of the TET2 catalytic domain eliminated the potency-enhancing effects of BET protein targeting in CAR T cells, providing a mechanism linking BET proteins and T cell dysfunction. Thus, modulating BET epigenetic readers may improve the efficacy of cell-based immunotherapies.
Keywords: Cancer gene therapy; Immunology; Leukemias; Oncology; T cells.
Conflict of interest statement
Figures
Similar articles
-
CD19 Chimeric Antigen Receptor T Cells From Patients With Chronic Lymphocytic Leukemia Display an Elevated IFN-γ Production Profile.J Immunother. 2018 Feb/Mar;41(2):73-83. doi: 10.1097/CJI.0000000000000193. J Immunother. 2018. PMID: 29315094 Free PMC article.
-
Current State of CAR T-Cell Therapy in Chronic Lymphocytic Leukemia.Int J Mol Sci. 2021 May 24;22(11):5536. doi: 10.3390/ijms22115536. Int J Mol Sci. 2021. PMID: 34073911 Free PMC article. Review.
-
Determinants of response and resistance to CD19 chimeric antigen receptor (CAR) T cell therapy of chronic lymphocytic leukemia.Nat Med. 2018 May;24(5):563-571. doi: 10.1038/s41591-018-0010-1. Epub 2018 Apr 30. Nat Med. 2018. PMID: 29713085 Free PMC article.
-
Disruption of TET2 promotes the therapeutic efficacy of CD19-targeted T cells.Nature. 2018 Jun;558(7709):307-312. doi: 10.1038/s41586-018-0178-z. Epub 2018 May 30. Nature. 2018. PMID: 29849141 Free PMC article.
-
Chimeric Antigen Receptor T Cell Therapy for Pediatric B-ALL: Narrowing the Gap Between Early and Long-Term Outcomes.Front Immunol. 2020 Aug 11;11:1985. doi: 10.3389/fimmu.2020.01985. eCollection 2020. Front Immunol. 2020. PMID: 32849662 Free PMC article. Review.
Cited by
-
A Review of CAR-T Combination Therapies for Treatment of Gynecological Cancers.Int J Mol Sci. 2024 Jun 15;25(12):6595. doi: 10.3390/ijms25126595. Int J Mol Sci. 2024. PMID: 38928301 Free PMC article. Review.
-
Fundamentals to therapeutics: Epigenetic modulation of CD8+ T Cell exhaustion in the tumor microenvironment.Front Cell Dev Biol. 2023 Jan 4;10:1082195. doi: 10.3389/fcell.2022.1082195. eCollection 2022. Front Cell Dev Biol. 2023. PMID: 36684449 Free PMC article. Review.
-
T-cell exhaustion and stemness in antitumor immunity: Characteristics, mechanisms, and implications.Front Immunol. 2023 Feb 20;14:1104771. doi: 10.3389/fimmu.2023.1104771. eCollection 2023. Front Immunol. 2023. PMID: 36891319 Free PMC article. Review.
-
Cytokine signaling in chimeric antigen receptor T-cell therapy.Int Immunol. 2024 Feb 14;36(2):49-56. doi: 10.1093/intimm/dxad033. Int Immunol. 2024. PMID: 37591521 Free PMC article. Review.
-
Chimeric Antigen Receptor T cell Therapy and the Immunosuppressive Tumor Microenvironment in Pediatric Sarcoma.Cancers (Basel). 2021 Sep 20;13(18):4704. doi: 10.3390/cancers13184704. Cancers (Basel). 2021. PMID: 34572932 Free PMC article. Review.
