

Clinical and perinatal outcomes of fresh single-blastocyst-transfer cycles under an early follicular phase prolonged protocol according to day of trigger estradiol levels
- PMID: 34395072
- PMCID: PMC8320517
- DOI: 10.7717/peerj.11785
Clinical and perinatal outcomes of fresh single-blastocyst-transfer cycles under an early follicular phase prolonged protocol according to day of trigger estradiol levels
Abstract
Backgroud: This study's objectives were to compare the clinical, perinatal, and obstetrical outcomes of patients with different estradiol (E2) levels in fresh single-blastocyst-transfer (SBT) cycles under an early follicular phase prolonged regimen on the day of trigger.
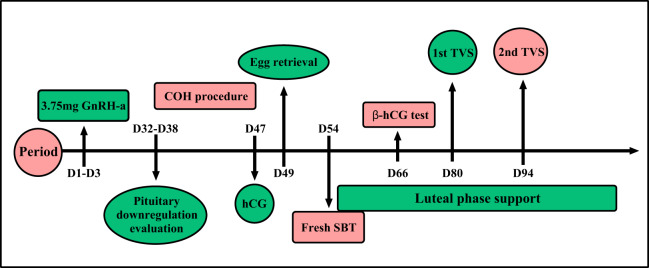
Methods: We recruited patients in fresh SBT cycles (n = 771) undergoing early follicular phase prolonged protocols with β-hCG values above 10 IU/L between June 2016 and December 2018. Patients who met the inclusion and exclusion criteria were divided into four groups according to their serum E2 level percentages on the day of trigger: <25th, 25th-50th, 51st-75th, and >75th percentile groups.
Results: Although the rates of clinical pregnancy (85.57% (166/194)), embryo implantation 86.60% (168/194), ongoing pregnancy (71.13% (138/194)), and live birth (71.13% (138/194)) were lowest in the >75th percentile group, we did not observe any significant differences (all P > 0.05). We used this information to predict the rate of severe ovarian hyperstimulation syndrome (OHSS) area under the curve (AUC) = 72.39%, P = 0.029, cut off value of E2 = 2,893 pg/ml with the 75% sensitivity and 70% specificity. The 51st-75th percentile group had the highest rates of low birth weight infants (11.73% (19/162), P = 0.0408), premature delivery (11.43% (20/175), P = 0.0269), admission to the neonatal intensive care unit (NICU) (10.49% (17/162), P = 0.0029), twin pregnancies (8.57% (15/175), P = 0.0047), and monochorionic diamniotic pregnancies (8.57% (15/175); P = 0.001). We did not observe statistical differences in obstetrics complications, including gestational diabetes mellitus (GDM), gestational hypertension, placenta previa, premature rupture of membranes (PROM), and preterm premature rupture of membranes (PPROM).
Conclusion: We concluded that serum E2 levels on the day of trigger were not good predictors of live birth rate or perinatal and obstetrical outcomes. However, we found that high E2 levels may not be conducive to persistent pregnancies. The E2 level on the day of trigger can still be used to predict the incidence of early onset severe OHSS in the fresh SBT cycle.
Keywords: Early follicular phase prolonged protocol; Estradiol level; Fresh single blastocyst transfer; Live birth; Perinatal outcome.
© 2021 Ying et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Length of estradiol exposure >100 pg/ml in the follicular phase affects pregnancy outcomes in natural frozen embryo transfer cycles.Hum Reprod. 2021 Jun 18;36(7):1932-1940. doi: 10.1093/humrep/deab111. Hum Reprod. 2021. PMID: 34128044
-
Slightly Elevated Progesterone on HCG Trigger Day Has an Impact on Pregnancy Outcomes of Fresh Single Blastocyst Transfer Cycles Under an Early Follicular Phase Prolonged Protocol Cycle.Int J Womens Health. 2022 Dec 19;14:1761-1768. doi: 10.2147/IJWH.S385362. eCollection 2022. Int J Womens Health. 2022. PMID: 36568124 Free PMC article.
-
Effect of progesterone/estradiol ratio on pregnancy outcome of patients with high trigger-day progesterone levels undergoing gonadotropin-releasing hormone antagonist intracytoplasmic sperm injection cycles: a retrospective cohort study.J Obstet Gynaecol. 2019 Feb;39(2):157-163. doi: 10.1080/01443615.2018.1504204. Epub 2018 Oct 3. J Obstet Gynaecol. 2019. PMID: 30280612
-
Influence of cryopreservation on perinatal outcome after blastocyst- vs cleavage-stage embryo transfer: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2018 Jan;51(1):54-63. doi: 10.1002/uog.18942. Ultrasound Obstet Gynecol. 2018. PMID: 29077229 Review.
-
GnRH Agonist Trigger and LH Activity Luteal Phase Support versus hCG Trigger and Conventional Luteal Phase Support in Fresh Embryo Transfer IVF/ICSI Cycles-A Systematic PRISMA Review and Meta-analysis.Front Endocrinol (Lausanne). 2017 Jun 7;8:116. doi: 10.3389/fendo.2017.00116. eCollection 2017. Front Endocrinol (Lausanne). 2017. PMID: 28638367 Free PMC article. Review.
Cited by
-
Elevated estradiol levels on hCG trigger day adversely effects on the clinical pregnancy rates of blastocyst embryo transfer but not cleavage-stage embryo transfer in fresh cycles: a retrospective cohort study.PeerJ. 2023 Jul 18;11:e15709. doi: 10.7717/peerj.15709. eCollection 2023. PeerJ. 2023. PMID: 37483963 Free PMC article.
-
E2 level > 2950 pg/ml on hCG trigger day is an independent predictor for birthweight loss of full-term singletons born after fresh embryo transfers in non-PCOS patients.Reprod Biol Endocrinol. 2022 Nov 21;20(1):162. doi: 10.1186/s12958-022-01027-9. Reprod Biol Endocrinol. 2022. PMID: 36411437 Free PMC article.
-
Which transfer day results in the highest live birth rate for PCOS patients undergoing in vitro fertilization?BMC Pregnancy Childbirth. 2023 Dec 16;23(1):865. doi: 10.1186/s12884-023-06173-5. BMC Pregnancy Childbirth. 2023. PMID: 38104082 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
