

Neutrophil-to-Lymphocyte Ratio as a Predictive Biomarker for Stroke Severity and Short-Term Prognosis in Acute Ischemic Stroke With Intracranial Atherosclerotic Stenosis
- PMID: 34393983
- PMCID: PMC8360230
- DOI: 10.3389/fneur.2021.705949
Neutrophil-to-Lymphocyte Ratio as a Predictive Biomarker for Stroke Severity and Short-Term Prognosis in Acute Ischemic Stroke With Intracranial Atherosclerotic Stenosis
Abstract
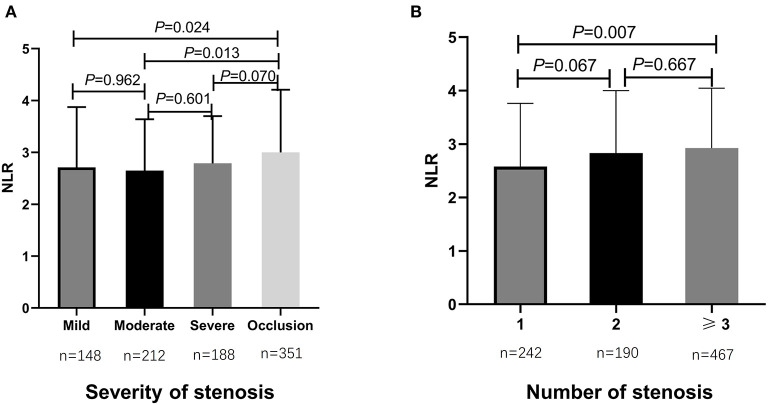
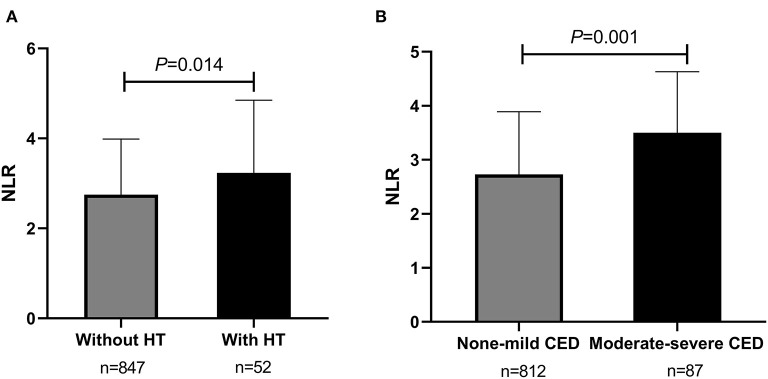
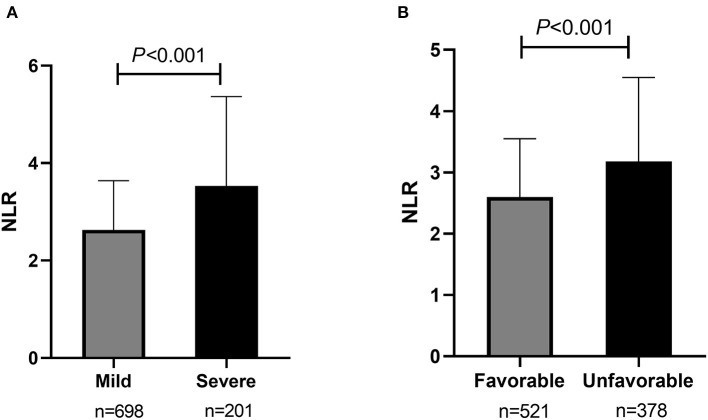
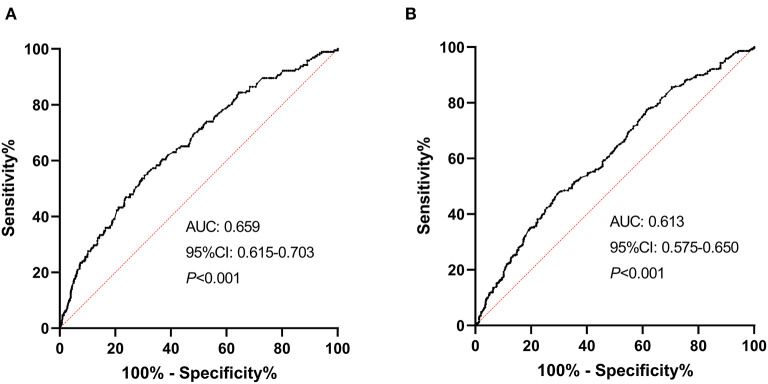
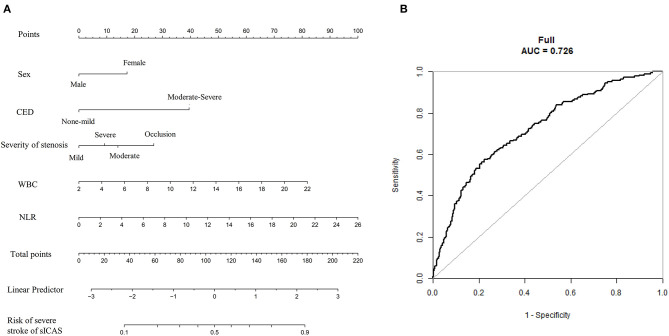
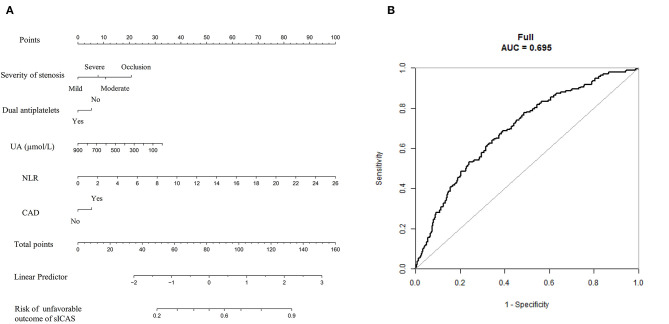
Background: Neutrophil-to-lymphocyte ratio (NLR) is an indicator of poor prognosis in acute ischemic stroke (AIS), but associations between NLR with stroke severity and prognosis of intracranial atherosclerotic stenosis (ICAS)-related ischemic events have not been well-elucidated; therefore, we aimed to evaluate whether admission NLR levels correlate with the early stroke severity and short-term functional prognosis in patients with symptomatic intracranial atherosclerotic stenosis (sICAS). Methods: This retrospective study enrolled 899 consecutive patients with AIS attributed to ICAS at Xiangya Hospital stroke center between May 2016 and September 2020. The initial stroke severity was rated by the admission National Institutes of Health Stroke Scale (NIHSS) scores, and the short-term prognosis was evaluated using the 14-day modified Rankin Scale (mRS) scores after stroke onset. A severe stroke was defined as NIHSS >8; an unfavorable functional outcome was defined as mRS scores of 3-6. Admission NLR was determined based on circulating neutrophil and lymphocyte counts. Results: The median admission NLR of all patients was 2.80 [interquartile range (IQR), 2.00-4.00]. In univariate analysis, admission NLR was significantly elevated in patients with severe stroke and poor short-term prognosis. After multivariate adjustment, admission NLR levels were significantly correlated with severe stroke [odds ratio (OR), 1.132; 95% confidence interval (95% CI), 1.038-1.234; P = 0.005] and unfavorable short-term prognosis (OR, 1.102; 95% CI, 1.017-1.195; P = 0.018) in Model 1. In Model 2, the highest NLR tertile (≥3.533) remained an independent predictor of severe stroke (OR, 2.736; 95% CI, 1.590-4.708; P < 0.001) and unfavorable functional outcome (OR, 2.165; 95% CI, 1.416-3.311; P < 0.001) compared with the lowest NLR tertile (<2.231). The receiver operating characteristic (ROC) curves showed the predictability of NLR regarding the stroke severity [area under the curve (AUC), 0.659; 95% CI, 0.615-0.703; P < 0.001] and short-term prognosis (AUC, 0.613; 95% CI, 0.575-0.650; P < 0.001). The nomograms were constructed to create the predictive models of the severity and short-term outcome of sICAS. Conclusions: Elevated admission NLR levels were independently associated with the initial stroke severity and could be an early predictor of severity and poor short-term prognosis in AIS patients with ICAS, which might help us identify a target group timely for preventive therapies.
Keywords: intracranial atherosclerotic stenosis; ischemic stroke; neutrophil-to-lymphocyte ratio; short-term prognosis; stroke severity.
Copyright © 2021 Ying, Yu, Luo, Feng, Liao, Wei, Li, Huang, Liu, Zhang, Zhao, Tu and Xia.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Low-normal free triiodothyronine and high leukocyte levels in relation to stroke severity and poor outcome in acute ischemic stroke with intracranial atherosclerotic stenosis.Int J Neurosci. 2019 Jul;129(7):635-641. doi: 10.1080/00207454.2018.1503179. Epub 2019 Feb 6. Int J Neurosci. 2019. PMID: 30251575
-
High neutrophil-to-lymphocyte ratio is a predictor of poor short-term outcome in patients with mild acute ischemic stroke receiving intravenous thrombolysis.Brain Behav. 2020 Dec;10(12):e01857. doi: 10.1002/brb3.1857. Epub 2020 Sep 27. Brain Behav. 2020. PMID: 32981201 Free PMC article.
-
High Neutrophil-Lymphocyte Ratio and Low Lymphocyte-Monocyte Ratio Combination after Thrombolysis Is a Potential Predictor of Poor Functional Outcome of Acute Ischemic Stroke.J Pers Med. 2022 Jul 27;12(8):1221. doi: 10.3390/jpm12081221. J Pers Med. 2022. PMID: 35893315 Free PMC article.
-
Neutrophil-lymphocyte ratio in acute ischemic stroke: Immunopathology, management, and prognosis.Acta Neurol Scand. 2021 Nov;144(5):486-499. doi: 10.1111/ane.13493. Epub 2021 Jun 30. Acta Neurol Scand. 2021. PMID: 34190348 Review.
-
The predictive role of the neutrophil-lymphocyte ratio in the prognosis of adult patients with stroke.Chin Neurosurg J. 2020 Jul 1;6:22. doi: 10.1186/s41016-020-00201-5. eCollection 2020. Chin Neurosurg J. 2020. PMID: 32922951 Free PMC article. Review.
Cited by
-
Efgartigimod versus intravenous immunoglobulin in the treatment of patients with impending myasthenic crisis.Sci Rep. 2024 Nov 18;14(1):28394. doi: 10.1038/s41598-024-79918-7. Sci Rep. 2024. PMID: 39551862 Free PMC article.
-
Associations of neutrophil-to-lymphocyte ratio with intracranial and extracranial atherosclerotic stenosis.Front Neurol. 2022 Sep 20;13:966022. doi: 10.3389/fneur.2022.966022. eCollection 2022. Front Neurol. 2022. PMID: 36203981 Free PMC article.
-
The Role of Preoperative Neutrophil, Platelet, and Monocyte to Lymphocyte Ratios as Independent Prognostic Factors for Patient Survival in WHO 2021 Glioblastoma: A Single-Center Retrospective Study.Cureus. 2022 Jun 9;14(6):e25801. doi: 10.7759/cureus.25801. eCollection 2022 Jun. Cureus. 2022. PMID: 35822134 Free PMC article.
-
Neutrophils and Platelets: Immune Soldiers Fighting Together in Stroke Pathophysiology.Biomedicines. 2021 Dec 19;9(12):1945. doi: 10.3390/biomedicines9121945. Biomedicines. 2021. PMID: 34944761 Free PMC article. Review.
-
Poststroke neutrophil count is predictive of the outcomes of large-artery atherosclerotic stroke and associated with craniocervical atherosclerosis.Sci Rep. 2023 Jul 17;13(1):11486. doi: 10.1038/s41598-023-37815-5. Sci Rep. 2023. PMID: 37460533 Free PMC article.
References
LinkOut - more resources
Full Text Sources