

The molecular etiology and treatment of glucocorticoid-induced osteoporosis
- PMID: 34386357
- PMCID: PMC8323641
- DOI: 10.4103/tcmj.tcmj_233_20
The molecular etiology and treatment of glucocorticoid-induced osteoporosis
Abstract
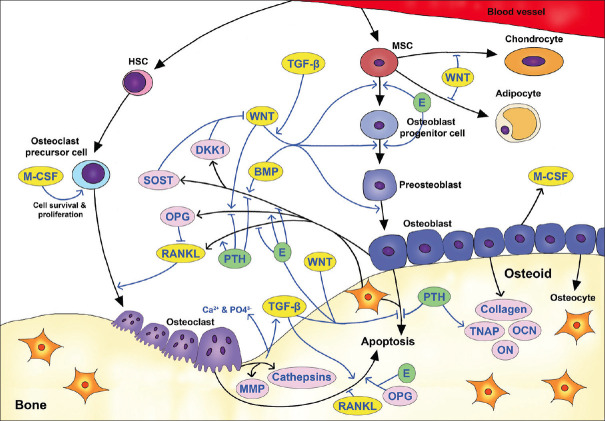
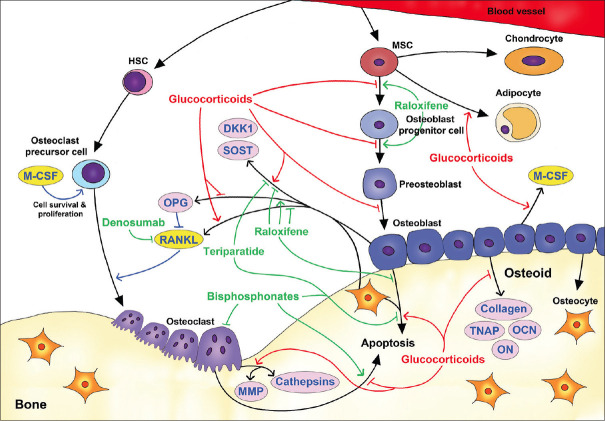
Glucocorticoid-induced osteoporosis (GIOP) is the most common form of secondary osteoporosis, accounting for 20% of osteoporosis diagnoses. Using glucocorticoids for >6 months leads to osteoporosis in 50% of patients, resulting in an increased risk of fracture and death. Osteoblasts, osteocytes, and osteoclasts work together to maintain bone homeostasis. When bone formation and resorption are out of balance, abnormalities in bone structure or function may occur. Excess glucocorticoids disrupt the bone homeostasis by promoting osteoclast formation and prolonging osteoclasts' lifespan, leading to an increase in bone resorption. On the other hand, glucocorticoids inhibit osteoblasts' formation and facilitate apoptosis of osteoblasts and osteocytes, resulting in a reduction of bone formation. Several signaling pathways, signaling modulators, endocrines, and cytokines are involved in the molecular etiology of GIOP. Clinically, adults ≥40 years of age using glucocorticoids chronically with a high fracture risk are considered to have medical intervention. In addition to vitamin D and calcium tablet supplementations, the major therapeutic options approved for GIOP treatment include antiresorption drug bisphosphonates, parathyroid hormone N-terminal fragment teriparatide, and the monoclonal antibody denosumab. The selective estrogen receptor modulator can only be used under specific condition for postmenopausal women who have GIOP but fail to the regular GIOP treatment or have specific therapeutic contraindications. In this review, we focus on the molecular etiology of GIOP and the molecular pharmacology of the therapeutic drugs used for GIOP treatment.
Keywords: Bone remodeling; Glucocorticoid; Osteoblast; Osteoclast; Secondary osteoporosis.
Copyright: © 2021 Tzu Chi Medical Journal.
Conflict of interest statement
Dr. Ing-Ho Chen, an editorial board member at Tzu Chi Medical Journal, had no roles in the peer review process of or decision to publish this article. The other authors declared that they have no conflicts of interest.
Figures
Similar articles
-
Osteoporosis Due to Hormone Imbalance: An Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover.Int J Mol Sci. 2022 Jan 25;23(3):1376. doi: 10.3390/ijms23031376. Int J Mol Sci. 2022. PMID: 35163300 Free PMC article. Review.
-
[Mechanisms and therapeutics of glucocorticoid-induced osteoporosis].Nihon Rinsho Meneki Gakkai Kaishi. 2011;34(3):138-48. doi: 10.2177/jsci.34.138. Nihon Rinsho Meneki Gakkai Kaishi. 2011. PMID: 21720102 Review. Japanese.
-
Management of glucocorticoids-induced osteoporosis: role of teriparatide.Ther Clin Risk Manag. 2009 Apr;5(2):305-10. doi: 10.2147/tcrm.s3940. Epub 2009 May 4. Ther Clin Risk Manag. 2009. PMID: 19536312 Free PMC article.
-
Pro-inflammatory Cytokines: Cellular and Molecular Drug Targets for Glucocorticoid-induced-osteoporosis via Osteocyte.Curr Drug Targets. 2019;20(1):1-15. doi: 10.2174/1389450119666180405094046. Curr Drug Targets. 2019. PMID: 29618305 Review.
-
Glucocorticosteroid-induced spinal osteoporosis: scientific update on pathophysiology and treatment.Eur Spine J. 2006 Jul;15(7):1035-49. doi: 10.1007/s00586-005-0056-x. Eur Spine J. 2006. PMID: 16474946 Free PMC article. Review.
Cited by
-
Carbonic Anhydrase II Activators in Osteopetrosis Treatment: A Review.Curr Issues Mol Biol. 2023 Feb 6;45(2):1373-1386. doi: 10.3390/cimb45020089. Curr Issues Mol Biol. 2023. PMID: 36826034 Free PMC article. Review.
-
Expression of Renal Vitamin D and Phosphatonin-Related Genes in a Sheep Model of Osteoporosis.Animals (Basel). 2021 Dec 29;12(1):67. doi: 10.3390/ani12010067. Animals (Basel). 2021. PMID: 35011173 Free PMC article.
-
The effect of Rutin hydrate on Glucocorticoids induced osteoporosis in mandibular alveolar bone in Albino rats (Radiological, histological and histochemical study).Saudi Dent J. 2022 Sep;34(6):464-472. doi: 10.1016/j.sdentj.2022.06.009. Epub 2022 Jun 28. Saudi Dent J. 2022. PMID: 36092520 Free PMC article.
-
A bibliometric and visualization analysis of glucocorticoid-induced osteoporosis research from 2012 to 2021.Front Endocrinol (Lausanne). 2022 Aug 5;13:961471. doi: 10.3389/fendo.2022.961471. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35992120 Free PMC article.
-
Geniposide Ameliorated Dexamethasone-Induced Cholesterol Accumulation in Osteoblasts by Mediating the GLP-1R/ABCA1 Axis.Cells. 2021 Dec 6;10(12):3424. doi: 10.3390/cells10123424. Cells. 2021. PMID: 34943934 Free PMC article.
References
-
- Wade SW, Strader C, Fitzpatrick LA, Anthony MS, O'Malley CD. Estimating prevalence of osteoporosis: Examples from industrialized countries. Arch Osteoporos. 2014;9:182. - PubMed
-
- Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J, et al. Osteoporosis in the European Union: Medical management, epidemiology and economic burden.A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA) Arch Osteoporos. 2013;8:136. - PMC - PubMed
-
- Odén A, McCloskey EV, Johansson H, Kanis JA. Assessing the impact of osteoporosis on the burden of hip fractures. Calcif Tissue Int. 2013;92:42–9. - PubMed
-
- Watts NB GLOW investigators. Insights from the Global Longitudinal Study of Osteoporosis in Women (GLOW) Nat Rev Endocrinol. 2014;10:412–22. - PubMed
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726–33. - PubMed
Publication types
LinkOut - more resources
Full Text Sources