

Predicted limited redistribution of T cells to secondary lymphoid tissue correlates with increased risk of haematological malignancies in asplenic patients
- PMID: 34385480
- PMCID: PMC8360980
- DOI: 10.1038/s41598-021-95225-x
Predicted limited redistribution of T cells to secondary lymphoid tissue correlates with increased risk of haematological malignancies in asplenic patients
Abstract
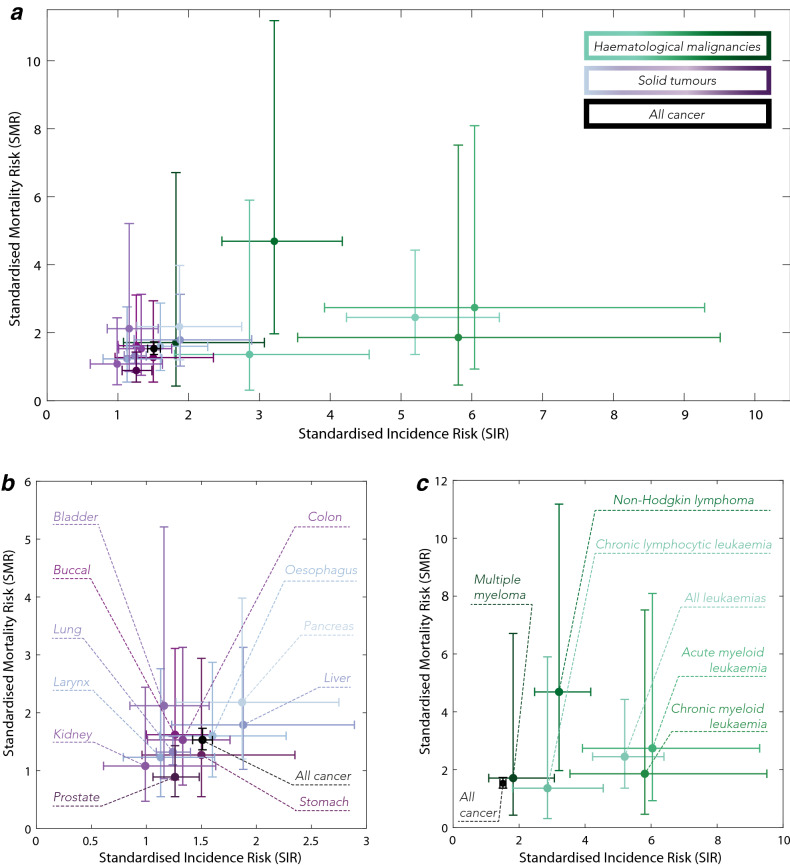
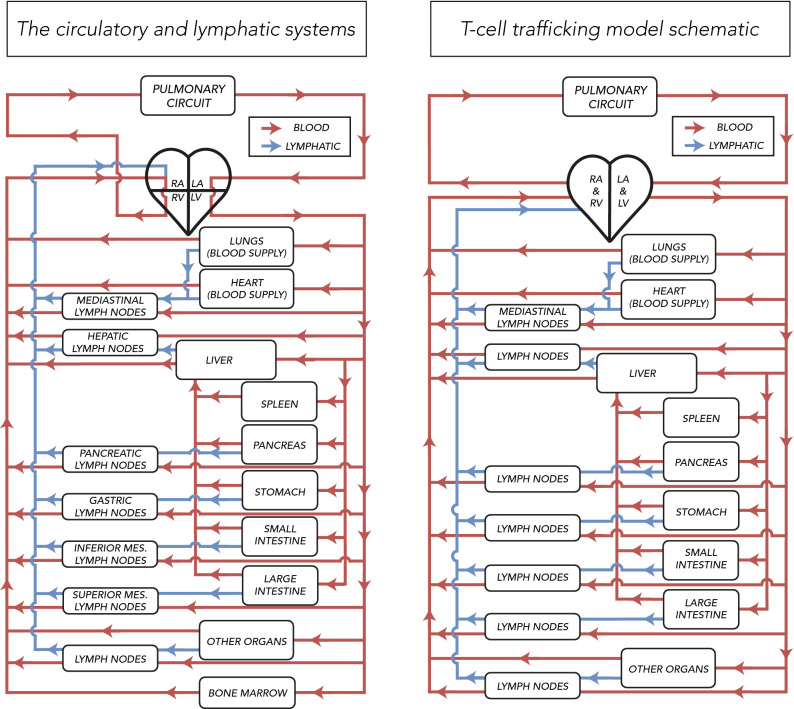
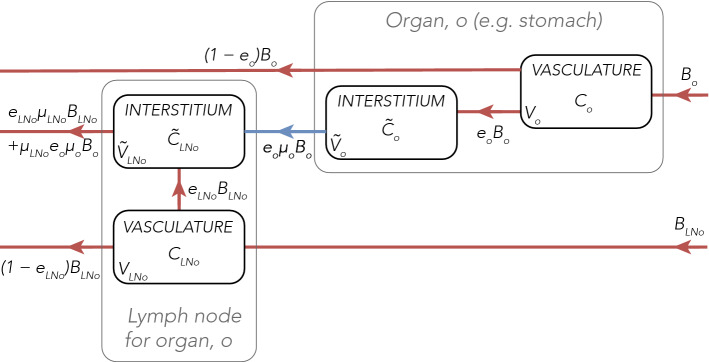
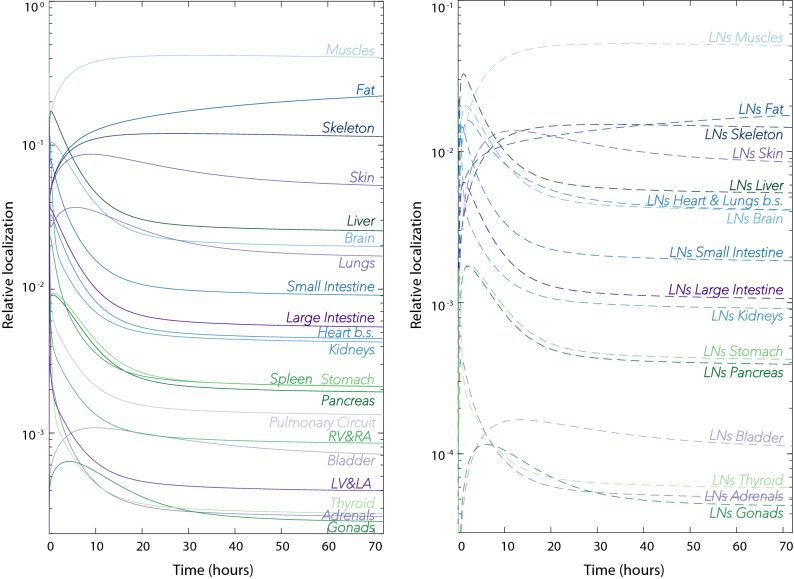
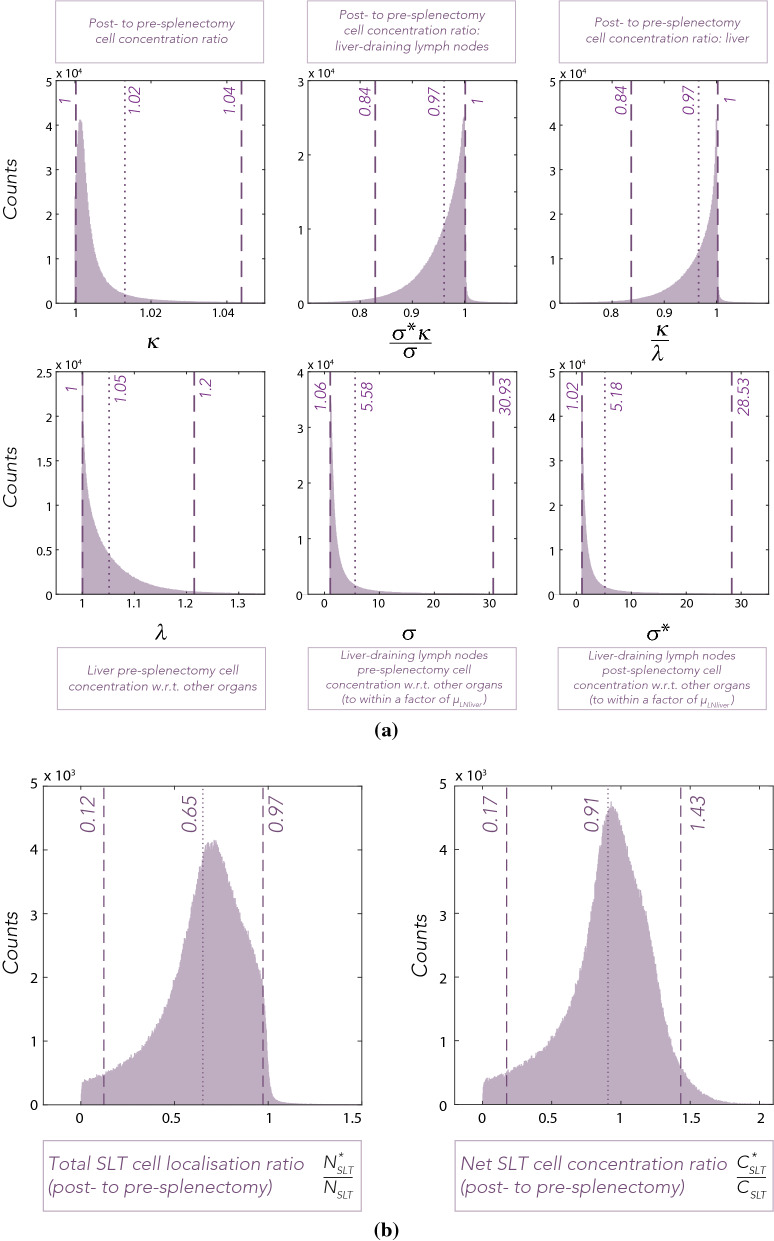
The spleen, a secondary lymphoid tissue (SLT), has an important role in generation of adaptive immune responses. Although splenectomy remains a common procedure, recent studies reported poor prognosis and increased risk of haematological malignancies in asplenic patients. The high baseline trafficking of T lymphocytes to splenic tissue suggests splenectomy may lead to loss of blood-borne malignant immunosurveillance that is not compensated for by the remaining SLT. To date, no quantitative analysis of the impact of splenectomy on the human T cell trafficking dynamics and tissue localisation has been reported. We developed a quantitative computational model that describes organ distribution and trafficking of human lymphocytes to explore the likely impact of splenectomy on immune cell distributions. In silico splenectomy resulted in an average reduction of T cell numbers in SLT by 35% (95%CI 0.12-0.97) and a comparatively lower, 9% (95%CI 0.17-1.43), mean decrease of T cell concentration in SLT. These results suggest that the surveillance capacity of the remaining SLT insufficiently compensates for the absence of the spleen. This may, in part, explain haematological malignancy risk in asplenic patients and raises the question of whether splenectomy has a clinically meaningful impact on patient responses to immunotherapy.
© 2021. The Author(s).
Conflict of interest statement
L.V.B, M.C.C. and E.A.G. declare no competing interests. At the time the work presented in this manuscript was completed, A.P. and J.W. were employees of and shareholders in F. Hoffmann-La Roche AG. F. Hoffmann-La Roche AG have contributed to the costs of the doctoral student, A.E.K., under the supervision of E.A.G. and M.C.C.
Figures
Similar articles
-
Hyposplenism and T lymphocyte subpopulations in coeliac disease and after splenectomy.J Clin Lab Immunol. 1985 Jun;17(2):75-7. J Clin Lab Immunol. 1985. PMID: 3876446
-
[Comparative hematologic and immunologic studies of patients with splenectomy and spleen autotransplantation].Magy Seb. 2005 Apr;58(2):74-9. Magy Seb. 2005. PMID: 16018271 Hungarian.
-
Lymphocyte subsets in the blood. The influence of splenectomy, splenic autotransplantation, ageing, and the site of blood sampling on the number of B, T, CD4+, and CD8+ lymphocytes in the rat.Scand J Immunol. 1990 Mar;31(3):327-34. doi: 10.1111/j.1365-3083.1990.tb02775.x. Scand J Immunol. 1990. PMID: 2108488
-
Post-splenectomy and hyposplenic states.Lancet. 2011 Jul 2;378(9785):86-97. doi: 10.1016/S0140-6736(10)61493-6. Epub 2011 Apr 5. Lancet. 2011. PMID: 21474172 Review.
-
The microstructure of secondary lymphoid organs that support immune cell trafficking.Arch Histol Cytol. 2010;73(1):1-21. doi: 10.1679/aohc.73.1. Arch Histol Cytol. 2010. PMID: 21471663 Review.
Cited by
-
The compensatory role of T cells from lymph nodes in mice with splenectomy.J Cell Mol Med. 2024 May;28(10):e18363. doi: 10.1111/jcmm.18363. J Cell Mol Med. 2024. PMID: 38770891 Free PMC article.
References
-
- Miyasaka M, Hata E, Tohya K, Hayasaka H. Lymphocyte recirculation. Encycl. Immunobiol. 2016 doi: 10.1016/B978-0-12-374279-7.07013-2. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
