

Addressing an HIV cure in LMIC
- PMID: 34344423
- PMCID: PMC8330180
- DOI: 10.1186/s12977-021-00565-1
Addressing an HIV cure in LMIC
Abstract
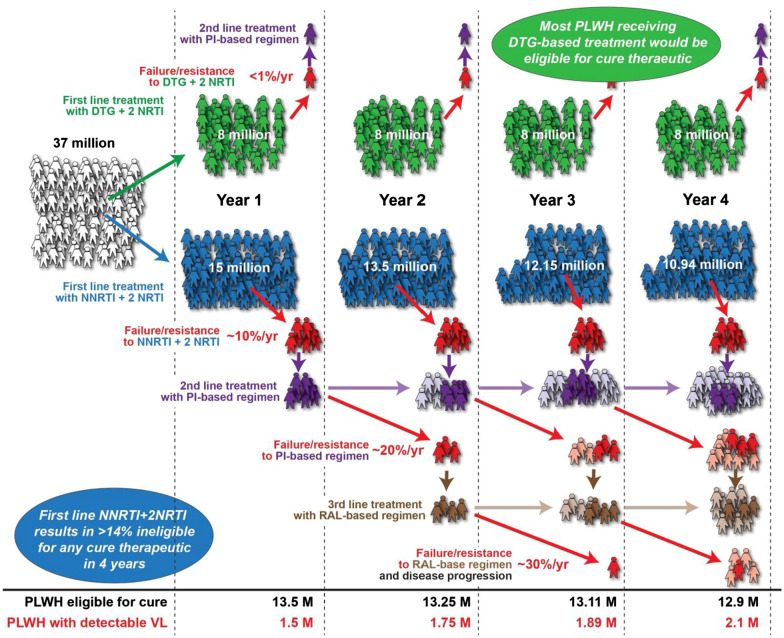
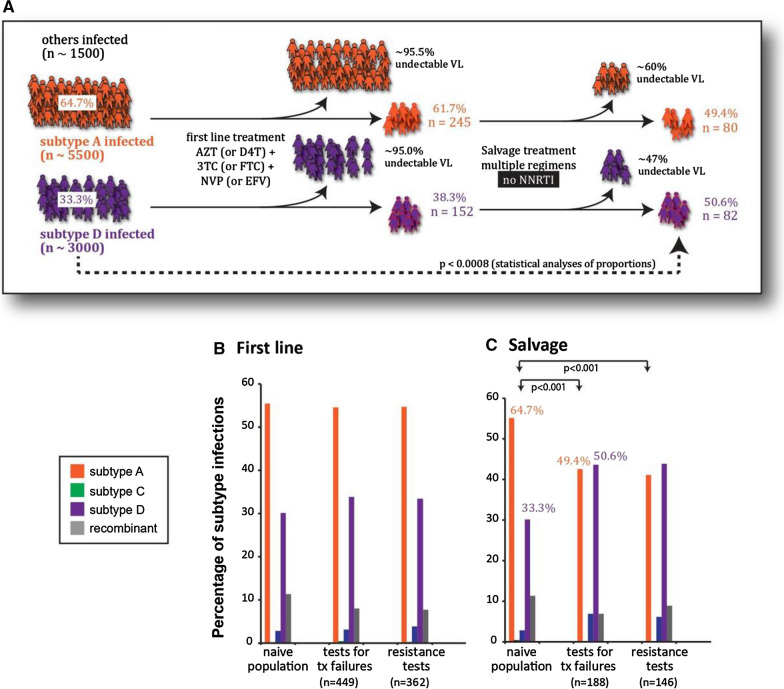
HIV-1 persists in infected individuals despite years of antiretroviral therapy (ART), due to the formation of a stable and long-lived latent viral reservoir. Early ART can reduce the latent reservoir and is associated with post-treatment control in people living with HIV (PLWH). However, even in post-treatment controllers, ART cessation after a period of time inevitably results in rebound of plasma viraemia, thus lifelong treatment for viral suppression is indicated. Due to the difficulties of sustained life-long treatment in the millions of PLWH worldwide, a cure is undeniably necessary. This requires an in-depth understanding of reservoir formation and dynamics. Differences exist in treatment guidelines and accessibility to treatment as well as social stigma between low- and-middle income countries (LMICs) and high-income countries. In addition, demographic differences exist in PLWH from different geographical regions such as infecting viral subtype and host genetics, which can contribute to differences in the viral reservoir between different populations. Here, we review topics relevant to HIV-1 cure research in LMICs, with a focus on sub-Saharan Africa, the region of the world bearing the greatest burden of HIV-1. We present a summary of ART in LMICs, highlighting challenges that may be experienced in implementing a HIV-1 cure therapeutic. Furthermore, we discuss current research on the HIV-1 latent reservoir in different populations, highlighting research in LMIC and gaps in the research that may facilitate a global cure. Finally, we discuss current experimental cure strategies in the context of their potential application in LMICs.
Keywords: Cure; HIV-1; LMICs; Low-and-middle income countries; Reservoir.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Plasma Viral Load of 200 Copies/mL is a Suitable Threshold to Define Viral Suppression and HIV Drug Resistance Testing in Low- and Middle-Income Countries: Evidence From a Facility-Based Study in Cameroon.J Int Assoc Provid AIDS Care. 2024 Jan-Dec;23:23259582241306484. doi: 10.1177/23259582241306484. J Int Assoc Provid AIDS Care. 2024. PMID: 39711049 Free PMC article.
-
Depressing time: Waiting, melancholia, and the psychoanalytic practice of care.In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. PMID: 36137063 Free Books & Documents. Review.
-
Community views on active case finding for tuberculosis in low- and middle-income countries: a qualitative evidence synthesis.Cochrane Database Syst Rev. 2024 Mar 21;3(3):CD014756. doi: 10.1002/14651858.CD014756.pub2. Cochrane Database Syst Rev. 2024. PMID: 38511668 Free PMC article. Review.
-
Effectiveness of interventions for improving educational outcomes for people with disabilities in low- and middle-income countries: A systematic review.Campbell Syst Rev. 2025 Feb 6;21(1):e70016. doi: 10.1002/cl2.70016. eCollection 2025 Mar. Campbell Syst Rev. 2025. PMID: 39917627 Free PMC article. Review.
-
The effectiveness of school-based family asthma educational programs on the quality of life and number of asthma exacerbations of children aged five to 18 years diagnosed with asthma: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):69-81. doi: 10.11124/jbisrir-2015-2335. JBI Database System Rev Implement Rep. 2015. PMID: 26571284
Cited by
-
High-resolution Inference of Multiplexed Anti-HIV Gene Editing using Single-Cell Targeted DNA Sequencing.bioRxiv [Preprint]. 2024 Aug 22:2024.01.24.576921. doi: 10.1101/2024.01.24.576921. bioRxiv. 2024. PMID: 38328062 Free PMC article. Preprint.
-
Reduced and highly diverse peripheral HIV-1 reservoir in virally suppressed patients infected with non-B HIV-1 strains in Uganda.Retrovirology. 2022 Jan 15;19(1):1. doi: 10.1186/s12977-022-00587-3. Retrovirology. 2022. PMID: 35033105 Free PMC article.
-
Advancing HIV cure research in low- and middle-income countries requires empowerment of the next generation of scientists.J Virus Erad. 2024 Mar 6;10(1):100364. doi: 10.1016/j.jve.2024.100364. eCollection 2024 Mar. J Virus Erad. 2024. PMID: 38559321 Free PMC article.
-
Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome-An Extempore Game of Misfiring with Defense Arsenals.Pathogens. 2023 Jan 29;12(2):210. doi: 10.3390/pathogens12020210. Pathogens. 2023. PMID: 36839482 Free PMC article. Review.
-
Effective and targeted latency reversal in CD4+ T cells from individuals on long term combined antiretroviral therapy initiated during chronic HIV-1 infection.Emerg Microbes Infect. 2024 Dec;13(1):2327371. doi: 10.1080/22221751.2024.2327371. Epub 2024 Mar 26. Emerg Microbes Infect. 2024. PMID: 38444369 Free PMC article.
References
-
- UNAIDS. Fact sheet—global AIDS update 2019. UNAIDS. 2019. https://www.unaids.org/en/resources/fact-sheet. Accessed 13 Apr 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
