

Understanding the Clinical Implications of Intracranial Arterial Calcification Using Brain CT and Vessel Wall Imaging
- PMID: 34335434
- PMCID: PMC8319500
- DOI: 10.3389/fneur.2021.619233
Understanding the Clinical Implications of Intracranial Arterial Calcification Using Brain CT and Vessel Wall Imaging
Abstract
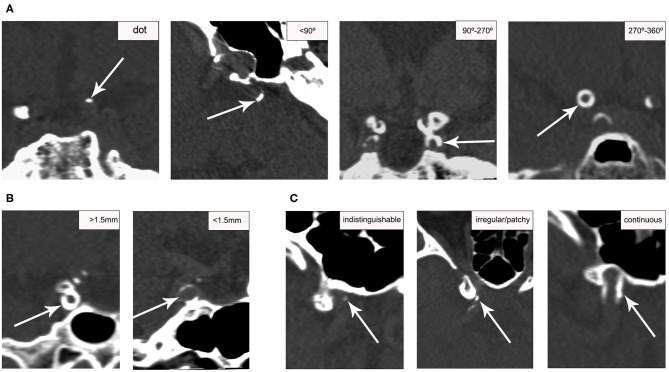
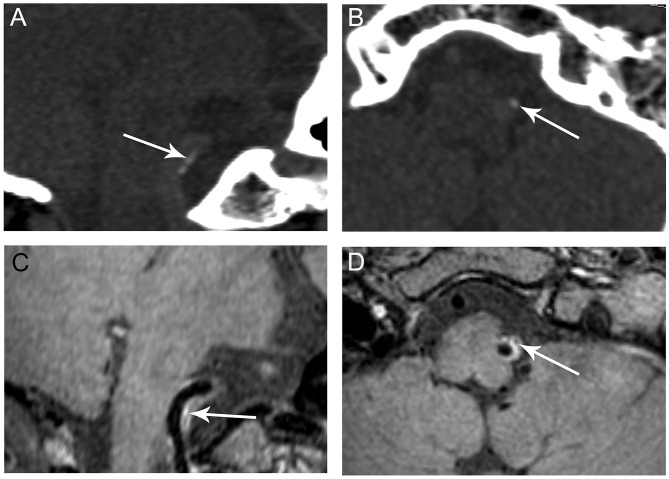
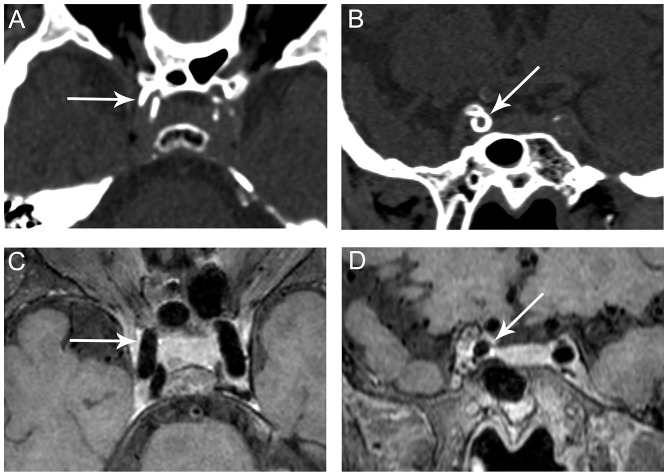
Background and Purpose: Intracranial arterial calcification (IAC) has been the focus of much attention by clinicians and researchers as an indicator of intracranial atherosclerosis, but correlations of IAC patterns (intimal or medial) with the presence of atherosclerotic plaques and plaque stability are still a matter of debate. Our study aimed to assess the associations of IAC patterns identified on computed tomography (CT) with the presence of plaque detected on vessel wall magnetic resonance imaging and plaque stability. Materials and Methods: Patients with stroke or transient ischemic attack and intracranial artery stenosis were recruited. IAC was detected and localized (intima or media) on non-contrast CT images. Intracranial atherosclerotic plaques were identified using vessel wall magnetic resonance imaging and matched to corresponding CT images. Associations between IAC patterns and culprit atherosclerotic plaques were assessed by using multivariate regression. Results: Seventy-five patients (mean age, 63.4 ± 11.6 years; males, 46) were included. Two hundred and twenty-one segments with IAC were identified on CT in 66 patients, including 86 (38.9%) predominantly intimal calcifications and 135 (61.1%) predominantly medial calcifications. A total of 72.0% of intimal calcifications coexisted with atherosclerotic plaques, whereas only 10.2% of medial calcifications coexisted with plaques. Intimal calcification was more commonly shown in non-culprit plaques than culprit plaques (25.9 vs. 9.4%, P = 0.008). The multivariate mixed logistic regression adjusted for the degree of stenosis showed that intimal calcification was significantly associated with non-culprit plaques (OR, 2.971; 95% CI, 1.036-8.517; P = 0.043). Conclusion: Our findings suggest that intimal calcification may indicate the existence of a stable form of atherosclerotic plaque, but plaques can exist in the absence of intimal calcification especially in the middle cerebral artery.
Keywords: atherosclerosis; calcification; computed tomography; intracranial disease; magnetic resonance imaging.
Copyright © 2021 Yang, Wasserman, Zheng, Huang, Li, Abrigo, Wong, Ying, Chu, Wong, Leung and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Intracranial Arterial Calcification and Intracranial Atherosclerosis: Close but Different.Front Neurol. 2022 Feb 8;13:799429. doi: 10.3389/fneur.2022.799429. eCollection 2022. Front Neurol. 2022. PMID: 35211084 Free PMC article.
-
Intimal predominant calcification is associated with plaque instability in the vertebrobasilar artery by vessel wall magnetic resonance imaging and computed tomography.Eur J Radiol. 2023 Nov;168:111132. doi: 10.1016/j.ejrad.2023.111132. Epub 2023 Oct 4. Eur J Radiol. 2023. PMID: 37806194
-
Postmortem Study Exploring Distribution and Patterns of Intracranial Artery Calcification.Stroke. 2018 Nov;49(11):2767-2769. doi: 10.1161/STROKEAHA.118.022591. Stroke. 2018. PMID: 30355206
-
Histology-Verified Intracranial Artery Calcification and Its Clinical Relevance With Cerebrovascular Disease.Front Neurol. 2022 Jan 24;12:789035. doi: 10.3389/fneur.2021.789035. eCollection 2021. Front Neurol. 2022. PMID: 35140673 Free PMC article. Review.
-
Calcium deposition within coronary atherosclerotic lesion: Implications for plaque stability.Atherosclerosis. 2020 Aug;306:85-95. doi: 10.1016/j.atherosclerosis.2020.05.017. Epub 2020 Jun 14. Atherosclerosis. 2020. PMID: 32654790 Review.
Cited by
-
Feasibility and intra-and interobserver reproducibility of quantitative susceptibility mapping with radiomic features for intracranial dissecting intramural hematomas and atherosclerotic calcifications.Sci Rep. 2023 Mar 4;13(1):3651. doi: 10.1038/s41598-023-30745-2. Sci Rep. 2023. PMID: 36871117 Free PMC article.
-
Epidemiology, Pathophysiology, and Imaging of Atherosclerotic Intracranial Disease.Stroke. 2024 Feb;55(2):311-323. doi: 10.1161/STROKEAHA.123.043630. Epub 2024 Jan 22. Stroke. 2024. PMID: 38252756 Review.
-
Intracranial Arterial Calcifications: Potential Biomarkers of Stroke Risk and Outcome.Front Neurol. 2022 Sep 1;13:900579. doi: 10.3389/fneur.2022.900579. eCollection 2022. Front Neurol. 2022. PMID: 36119671 Free PMC article. Review.
-
Vertebrobasilar Junction Angle Over 90°: A Potential Imaging Marker Associated With Vertebrobasilar Atherosclerosis.Front Neurosci. 2022 Jan 5;15:789852. doi: 10.3389/fnins.2021.789852. eCollection 2021. Front Neurosci. 2022. PMID: 35069103 Free PMC article.
-
The correlation between intracranial arterial calcification and the outcome of reperfusion therapy.Ann Clin Transl Neurol. 2023 Jun;10(6):974-982. doi: 10.1002/acn3.51780. Epub 2023 Apr 23. Ann Clin Transl Neurol. 2023. PMID: 37088543 Free PMC article.
References
LinkOut - more resources
Full Text Sources