

Effectiveness of a Multicomponent Intervention to Reduce Multidrug-Resistant Organisms in Nursing Homes: A Cluster Randomized Clinical Trial
- PMID: 34269807
- PMCID: PMC8285736
- DOI: 10.1001/jamanetworkopen.2021.16555
Effectiveness of a Multicomponent Intervention to Reduce Multidrug-Resistant Organisms in Nursing Homes: A Cluster Randomized Clinical Trial
Abstract
Importance: Multidrug-resistant organisms (MDROs) can cause significant morbidity and mortality. Preventing MDROs can reduce the risk of subsequent transmission and infection.
Objective: To determine whether a multicomponent infection prevention intervention can reduce MDRO prevalence in nursing homes (NHs).
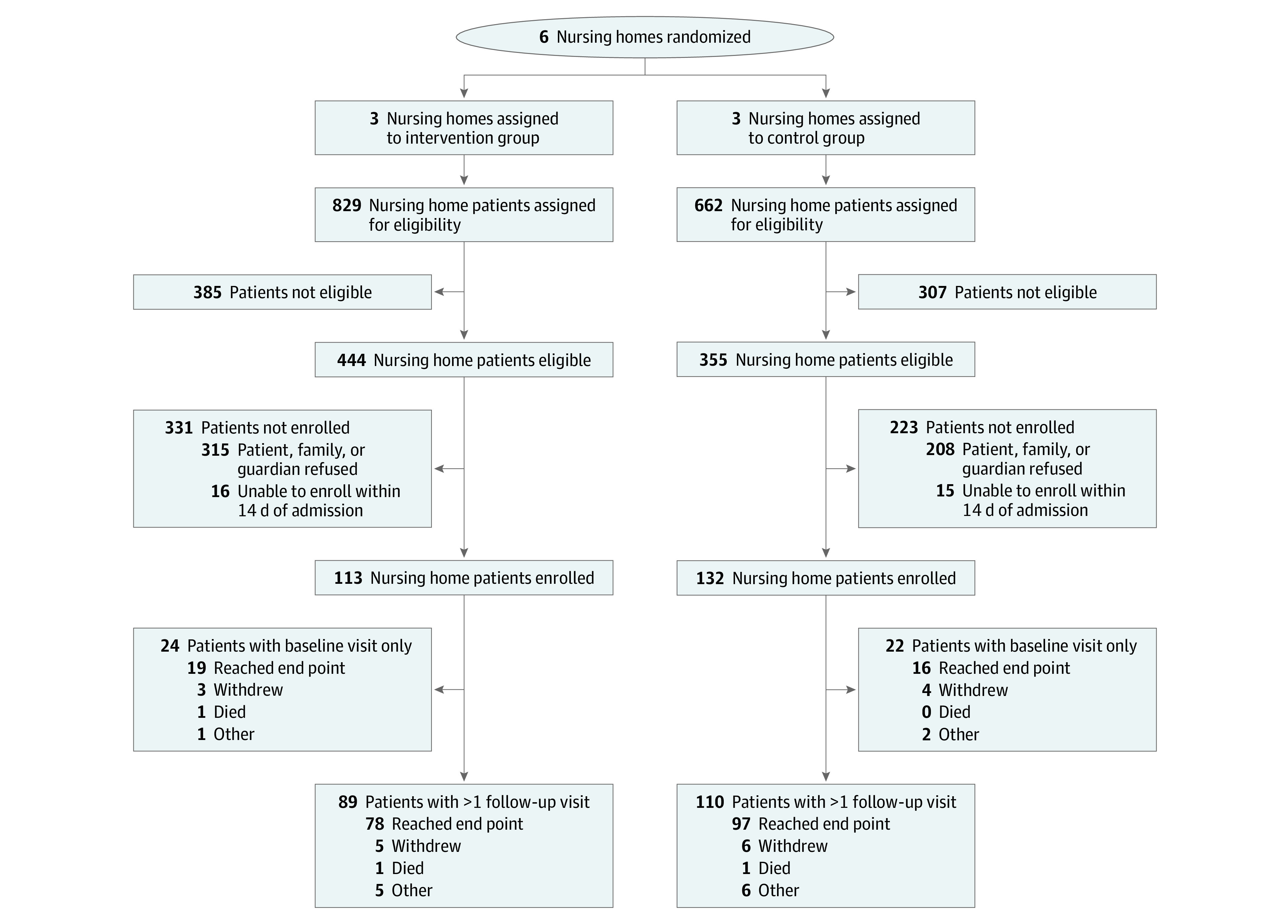
Design, setting, and participants: This cluster randomized clinical trial of a multicomponent intervention was conducted in 6 NHs in Michigan from September 2016 to August 2018. Three NHs adopted a multicomponent intervention, while 3 control NHs continued without investigator intervention. Study visits were conducted at baseline; days 7, 14, 21, and 30; and monthly thereafter for up to 6 months or discharge. Visits included clinical data collection and MDRO surveillance culturing of multiple body sites and high-touch surfaces in patient rooms. Any patients who provided informed consent within 14 days of admission to the NH were enrolled in this study. Non-English speakers and patients receiving hospice care were ineligible. Analysis was performed from November 2018 to February 2020.
Interventions: Intervention NHs adopted a multicomponent intervention that included enhanced barrier precautions, chlorhexidine bathing, MDRO surveillance, environmental cleaning education and feedback, hand hygiene promotion, and health care worker education and feedback. Control nursing homes continued standard care practices.
Main outcomes and measures: The primary outcome, presence of MDROs, was measured longitudinally in the patient and room environment and was evaluated using generalized mixed effect models. The secondary outcome, time to new MDRO acquisition, was assessed using Cox proportional hazard models.
Results: A total of 6 NHs were included, with 245 patients (mean [SD] age, 72.5 [13.6] years; 134 [54.7%] women) enrolled; 3 NHs with 113 patients (46.1%) were randomized to the intervention group and 3 NHs with 132 patients (53.9%) were randomized to the control group. A total of 132 patients (53.9%) were White, and 235 patients (95.9%) were receiving postacute care. Over 808 study visits, 3654 patient cultures and 5606 environmental cultures were obtained. The intervention reduced the odds of MDRO prevalence in patients' environment by 43% (aOR, 0.57; 95% CI, 0.35-0.94), but there was no statistically significant difference on the patient level before or after adjustment (aOR, 0.57; 95% CI, 0.29-1.14). There were no significant reductions in time to new acquisition for methicillin-resistant Staphylococcus aureus (hazard ratio [HR], 0.20; 95% CI, 0.04-1.09), vancomycin-resistant enterococci (HR, 0.84; 95% CI, 0.46-1.53), or resistant gram-negative bacilli (HR, 1.14; 95% CI, 0.73-1.78).
Conclusions and relevance: This cluster randomized clinical trial found that the multicomponent intervention reduced the prevalence of MDROs in the environment of NH patients. Our findings highlight the potential for multicomponent interventions to directly and indirectly reduce MDRO prevalence in NHs.
Trial registration: ClinicalTrials.gov Identifier: NCT02909946.
Conflict of interest statement
Figures
Similar articles
-
Approaches to multidrug-resistant organism prevention and control in long-term care facilities for older people: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2022 Jan 15;11(1):7. doi: 10.1186/s13756-021-01044-0. Antimicrob Resist Infect Control. 2022. PMID: 35033198 Free PMC article. Review.
-
A targeted infection prevention intervention in nursing home residents with indwelling devices: a randomized clinical trial.JAMA Intern Med. 2015 May;175(5):714-23. doi: 10.1001/jamainternmed.2015.132. JAMA Intern Med. 2015. PMID: 25775048 Free PMC article. Clinical Trial.
-
Reducing Hospitalizations and Multidrug-Resistant Organisms via Regional Decolonization in Hospitals and Nursing Homes.JAMA. 2024 May 14;331(18):1544-1557. doi: 10.1001/jama.2024.2759. JAMA. 2024. PMID: 38557703 Free PMC article.
-
Association of Exposure to High-risk Antibiotics in Acute Care Hospitals With Multidrug-Resistant Organism Burden in Nursing Homes.JAMA Netw Open. 2022 Feb 1;5(2):e2144959. doi: 10.1001/jamanetworkopen.2021.44959. JAMA Netw Open. 2022. PMID: 35103795 Free PMC article.
-
Hand and environmental hygiene: respective roles for MRSA, multi-resistant gram negatives, Clostridioides difficile, and Candida spp.Antimicrob Resist Infect Control. 2024 Sep 27;13(1):110. doi: 10.1186/s13756-024-01461-x. Antimicrob Resist Infect Control. 2024. PMID: 39334403 Free PMC article. Review.
Cited by
-
Prevention and control of hospital-acquired infections with multidrug-resistant organism: A review.Medicine (Baltimore). 2024 Jan 26;103(4):e37018. doi: 10.1097/MD.0000000000037018. Medicine (Baltimore). 2024. PMID: 38277558 Free PMC article. Review.
-
Bacterial infections epidemiology and factors associated with multidrug resistance in the northern region of Ghana.Sci Rep. 2022 Dec 21;12(1):22069. doi: 10.1038/s41598-022-26547-7. Sci Rep. 2022. PMID: 36543904 Free PMC article.
-
Approaches to multidrug-resistant organism prevention and control in long-term care facilities for older people: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2022 Jan 15;11(1):7. doi: 10.1186/s13756-021-01044-0. Antimicrob Resist Infect Control. 2022. PMID: 35033198 Free PMC article. Review.
-
A call to action: the SHEA research agenda to combat healthcare-associated infections.Infect Control Hosp Epidemiol. 2024 Oct 25;45(9):1-18. doi: 10.1017/ice.2024.125. Online ahead of print. Infect Control Hosp Epidemiol. 2024. PMID: 39448369 Free PMC article. No abstract available.
-
Bacterial contamination on used face masks among nursing home healthcare personnel.Antimicrob Steward Healthc Epidemiol. 2023 Mar 15;3(1):e54. doi: 10.1017/ash.2023.130. eCollection 2023. Antimicrob Steward Healthc Epidemiol. 2023. PMID: 36970428 Free PMC article.
References
-
- Safdar N, Maki DG. The commonality of risk factors for nosocomial colonization and infection with antimicrobial-resistant Staphylococcus aureus, Enterococcus, gram-negative bacilli, Clostridium difficile, and Candida. Ann Intern Med. 2002;136(11):834-844. doi:10.7326/0003-4819-136-11-200206040-00013 - DOI - PubMed
-
- Cassone M, Zhu Z, Mantey J, et al. . Interplay between patient colonization and environmental contamination with vancomycin-resistant Enterococci and their association with patient health outcomes in postacute care. Open Forum Infect Dis. 2019;7(1):ofz519. doi:10.1093/ofid/ofz519 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
