

Hypokalemic Periodic Paralysis Precipitated by Thyrotoxicosis and Renal Tubular Acidosis
- PMID: 34239739
- PMCID: PMC8238611
- DOI: 10.1155/2021/4529009
Hypokalemic Periodic Paralysis Precipitated by Thyrotoxicosis and Renal Tubular Acidosis
Abstract
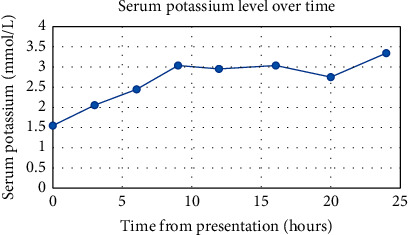
Background: Hypokalemic periodic paralysis is a rare neuromuscular disorder characterized by transient episodes of flaccid paralysis due to a defect in muscle ion channels. Most cases are hereditary, but it can be acquired. We present a case of acquired hypokalemic periodic paralysis associated with hyperthyroidism and renal tubular acidosis. Clinical Case. A 38-year-old female with a history of Graves' disease presented to the emergency department with generalized weakness and associated nausea, vomiting, and weight loss. Examination was significant for diffuse weakness in all extremities. Labs showed hypokalemia, hyperthyroidism, and nonanion gap metabolic acidosis with a positive urine anion gap. She was treated for hypokalemic periodic paralysis and renal tubular acidosis. Potassium replacement, propranolol, methimazole, and sodium bicarbonate were initiated. Her potassium gradually corrected with resolution of her symptoms. Further investigation revealed a history of dry eyes, dry mouth, and recurrent dental carries. She had positive ANA, SS-A, and SS-B antibodies. She was diagnosed with Sjögren's syndrome, which may have been associated with her Graves' disease and thus contributed to both her RTA and hyperthyroidism.
Conclusion: Early recognition and treatment of thyrotoxic periodic paralysis are important to prevent cardiac complications. Management includes potassium replacement with careful monitoring to prevent rebound hyperkalemia. The definitive treatment is to achieve euthyroid status.
Copyright © 2021 Ian Jackson et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Similar articles
-
Graves' Disease With Initial Presentation of Thyrotoxic Periodic Paralysis.Cureus. 2023 Nov 27;15(11):e49524. doi: 10.7759/cureus.49524. eCollection 2023 Nov. Cureus. 2023. PMID: 38156140 Free PMC article.
-
Clinical and Aetiological Spectrum of Hypokalemic Flaccid Paralysis in Western Odisha.J Assoc Physicians India. 2016 May;64(5):52-58. J Assoc Physicians India. 2016. PMID: 27735149
-
Hypokalemic periodic paralysis and renal tubular acidosis in a patient with hypothyroid and autoimmune disease.Ann Med Surg (Lond). 2022 Feb 22;75:103389. doi: 10.1016/j.amsu.2022.103389. eCollection 2022 Mar. Ann Med Surg (Lond). 2022. PMID: 35242331 Free PMC article.
-
Sjögren's syndrome presenting as hypokalemic periodic paralysis.Arthritis Rheum. 1993 Dec;36(12):1735-8. doi: 10.1002/art.1780361213. Arthritis Rheum. 1993. PMID: 8250993 Review.
-
Clinical review: Thyrotoxic periodic paralysis: a diagnostic challenge.J Clin Endocrinol Metab. 2006 Jul;91(7):2490-5. doi: 10.1210/jc.2006-0356. Epub 2006 Apr 11. J Clin Endocrinol Metab. 2006. PMID: 16608889 Review.
Cited by
-
Unusual presentation of Sjogren's syndrome during pregnancy: a case report.J Med Case Rep. 2024 May 4;18(1):236. doi: 10.1186/s13256-024-04563-7. J Med Case Rep. 2024. PMID: 38702803 Free PMC article.
-
Distal Renal Tubular Acidosis in Patients with Autoimmune Diseases-An Update on Pathogenesis, Clinical Presentation and Therapeutic Strategies.Biomedicines. 2022 Aug 31;10(9):2131. doi: 10.3390/biomedicines10092131. Biomedicines. 2022. PMID: 36140232 Free PMC article. Review.
-
A Rare Case of Hypokalemic Periodic Paralysis With Acute Urinary Retention: Diagnosis and Management.Cureus. 2024 Jan 24;16(1):e52839. doi: 10.7759/cureus.52839. eCollection 2024 Jan. Cureus. 2024. PMID: 38406120 Free PMC article.
-
The Aging Features of Thyrotoxicosis Mice: Malnutrition, Immunosenescence and Lipotoxicity.Front Immunol. 2022 Jun 2;13:864929. doi: 10.3389/fimmu.2022.864929. eCollection 2022. Front Immunol. 2022. PMID: 35720307 Free PMC article.
-
Primary Sjögren's syndrome complicated by renal tubular acidosis and acute bilateral uveitis: a case report and literature review.J Int Med Res. 2024 Nov;52(11):3000605241275880. doi: 10.1177/03000605241275880. J Int Med Res. 2024. PMID: 39568254 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
