

Role of Brain Arterial Remodeling in HIV-Associated Cerebrovascular Outcomes
- PMID: 34239489
- PMCID: PMC8258100
- DOI: 10.3389/fneur.2021.593605
Role of Brain Arterial Remodeling in HIV-Associated Cerebrovascular Outcomes
Abstract
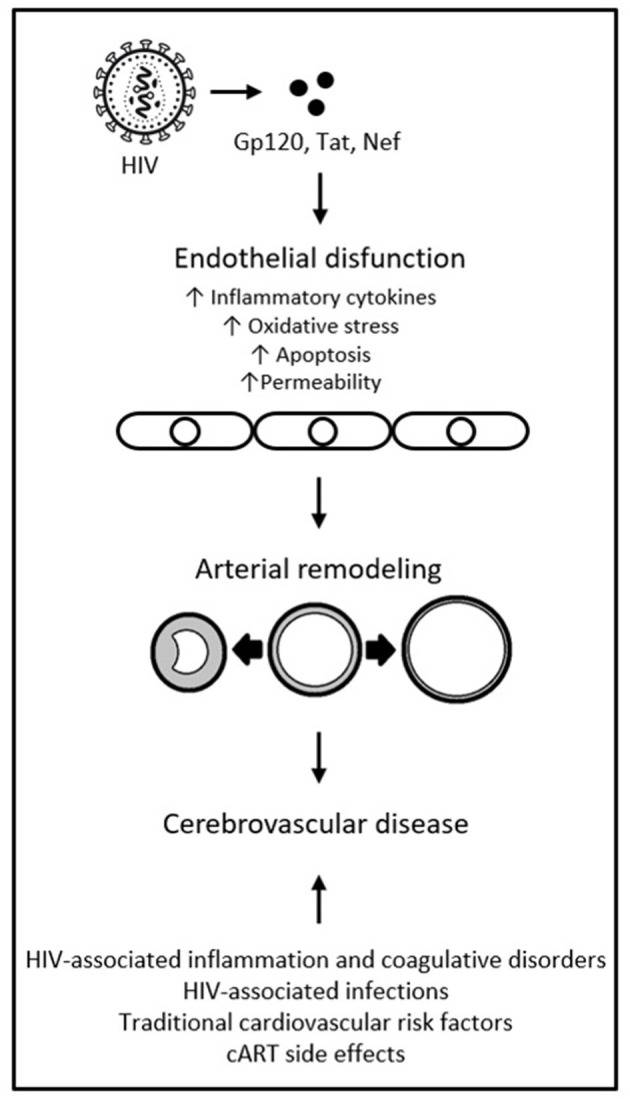
As the life expectancy of people living with HIV (PLWH) on combination antiretroviral therapy (cART) increases, so does morbidity from cerebrovascular disease and neurocognitive disorders. Brain arterial remodeling stands out as a novel investigational target to understand the role of HIV in cerebrovascular and neurocognitive outcomes. We therefore conducted a review of publications in PubMed, EMBASE, Web of Science and Wiley Online Library, from inception to April 2021. We included search terms such as HIV, cART, brain, neuroimmunity, arterial remodeling, cerebrovascular disease, and neurocognitive disorders. The literature shows that, in the post-cART era, PLWH continue to experience an increased risk of stroke and neurocognitive disorders (albeit milder forms) compared to uninfected populations. PLWH who are immunosuppressed have a higher proportion of hemorrhagic strokes and strokes caused by opportunistic infection and HIV vasculopathy, while PLWH on long-term cART have higher rates of ischemic strokes, compared to HIV-seronegative controls. Brain large artery atherosclerosis in PLWH is associated with lower CD4 nadir and higher CD4 count during the stroke event. HIV vasculopathy, a form of non-atherosclerotic outward remodeling, on the other hand, is associated with protracted immunosuppression. HIV vasculopathy was also linked to a thinner media layer and increased adventitial macrophages, suggestive of non-atherosclerotic degeneration of the brain arterial wall in the setting of chronic central nervous system inflammation. Cerebrovascular architecture seems to be differentially affected by HIV infection in successfully treated versus immunosuppressed PLWH. Brain large artery atherosclerosis is prevalent even with long-term immune reconstitution post-cART. HIV-associated changes in brain arterial walls may also relate to higher rates of HIV-associated neurocognitive disorders, although milder forms are more prevalent in the post-cART era. The underlying mechanisms of HIV-associated pathological arterial remodeling remain poorly understood, but a role has been proposed for chronic HIV-associated inflammation with increased burden on the vasculature. Neuroimaging may come to play a role in assessing brain arterial remodeling and stratifying cerebrovascular risk, but the data remains inconclusive. An improved understanding of the different phenotypes of brain arterial remodeling associated with HIV may reveal opportunities to reduce rates of cerebrovascular disease in the aging population of PLWH on cART.
Keywords: HIV; HIV-associated neurocognitive impairment; arterial remodeling; brain; cerebrovascular disease.
Copyright © 2021 Spagnolo-Allende and Gutierrez.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Brain Large Artery Lymphocytic Inflammation and Human Immunodeficiency Virus-Related Brain Arterial Remodeling.J Virol. 2018 May 29;92(12):e00081-18. doi: 10.1128/JVI.00081-18. Print 2018 Jun 15. J Virol. 2018. PMID: 29618649 Free PMC article.
-
Brain arterial remodeling contribution to nonembolic brain infarcts in patients with HIV.Neurology. 2015 Sep 29;85(13):1139-45. doi: 10.1212/WNL.0000000000001976. Epub 2015 Aug 28. Neurology. 2015. PMID: 26320196 Free PMC article.
-
Burden of subclinical carotid atherosclerosis and vascular risk factors among people living with HIV in Ghana.J Neurol Sci. 2019 Feb 15;397:103-111. doi: 10.1016/j.jns.2018.12.026. Epub 2018 Dec 19. J Neurol Sci. 2019. PMID: 30599299 Free PMC article.
-
Multimodal Approach to Neurocognitive Function in People Living with HIV in the cART Era: A Comprehensive Review.Life (Basel). 2024 Apr 15;14(4):508. doi: 10.3390/life14040508. Life (Basel). 2024. PMID: 38672778 Free PMC article. Review.
-
Changing clinical phenotypes of HIV-associated neurocognitive disorders.J Neurovirol. 2018 Apr;24(2):141-145. doi: 10.1007/s13365-017-0556-6. Epub 2017 Jul 27. J Neurovirol. 2018. PMID: 28752495 Free PMC article. Review.
Cited by
-
Exercise to Prevent Accelerated Vascular Aging in People Living With HIV.Circ Res. 2024 May 24;134(11):1607-1635. doi: 10.1161/CIRCRESAHA.124.323975. Epub 2024 May 23. Circ Res. 2024. PMID: 38781293 Review.
-
Altered mucosal immunity in HIV-positive colon adenoma: decreased CD4+ T cell infiltration is correlated with nadir but not current CD4+ T cell blood counts.Int J Clin Oncol. 2022 Aug;27(8):1321-1330. doi: 10.1007/s10147-022-02188-8. Epub 2022 May 29. Int J Clin Oncol. 2022. PMID: 35643870
-
New Directions in Infection-Associated Ischemic Stroke.J Clin Neurol. 2024 Mar;20(2):140-152. doi: 10.3988/jcn.2023.0056. Epub 2024 Feb 5. J Clin Neurol. 2024. PMID: 38330416 Free PMC article. Review.
References
-
- Deeks SG. Immune dysfunction, inflammation, and accelerated aging in patients on antiretroviral therapy. Top HIV Med. (2009) 17:118–23. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous