

Metabolic profile of heart tissue in cyanotic congenital heart disease
- PMID: 34150010
- PMCID: PMC8205768
Metabolic profile of heart tissue in cyanotic congenital heart disease
Abstract
Background: Cyanotic congenital heart disease (CCHD) is one of the most common birth anomalies, in which chronic hypoxia is the basic pathophysiological process.
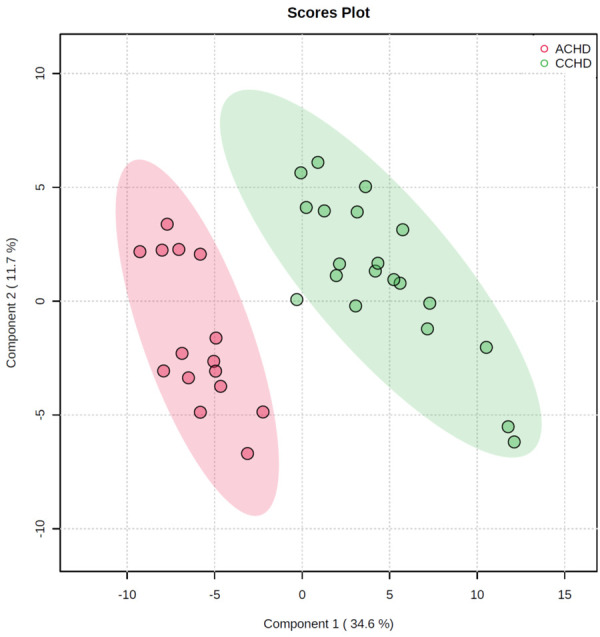
Methods: To investigate the heart's metabolic remodeling to hypoxia, we performed an untargeted metabolomic analysis of cardiac tissue from 20 CCHD patients and 15 patients with acyanotic congenital heart disease (ACHD).
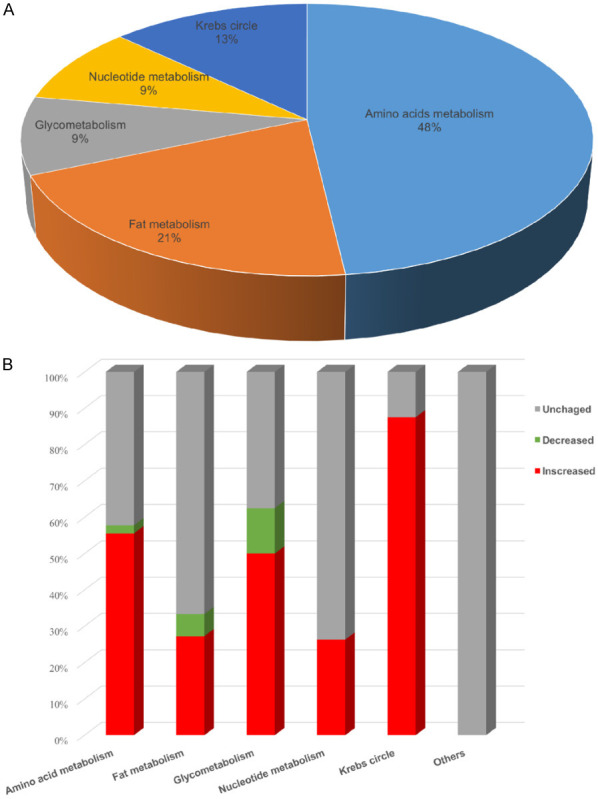
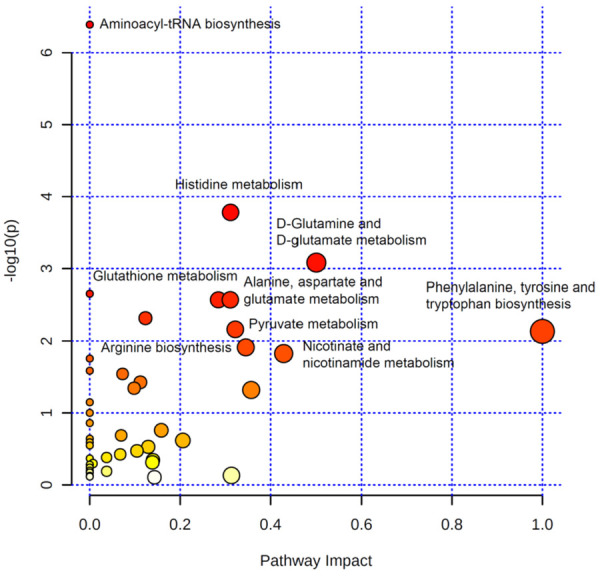
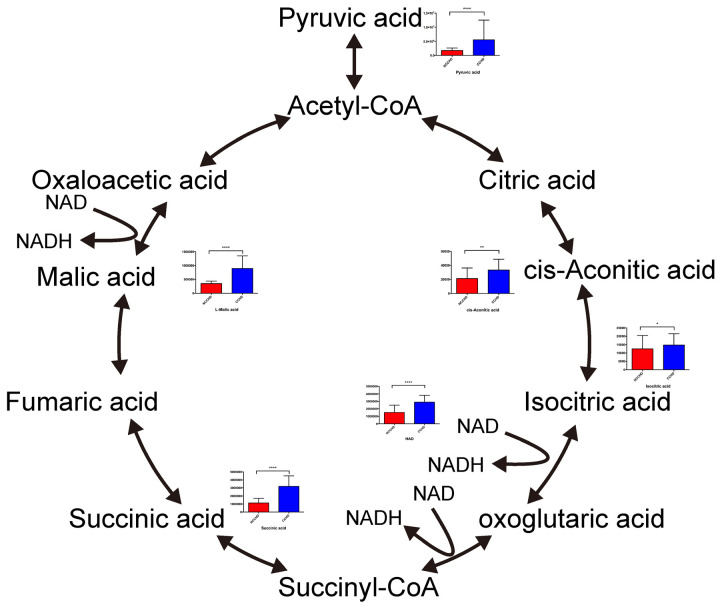
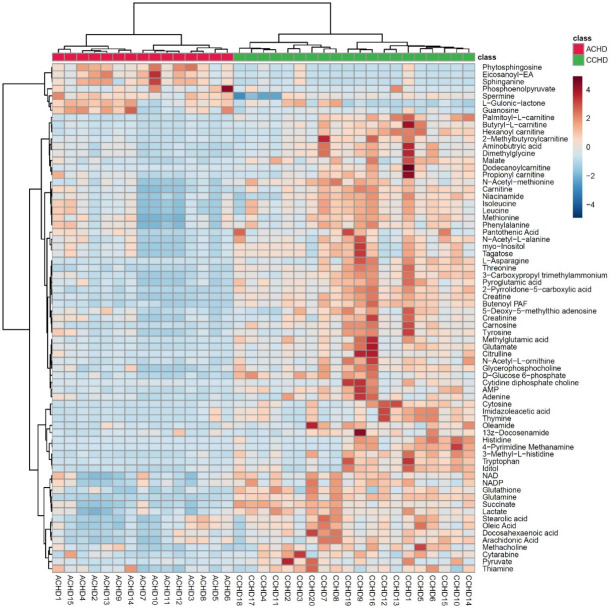
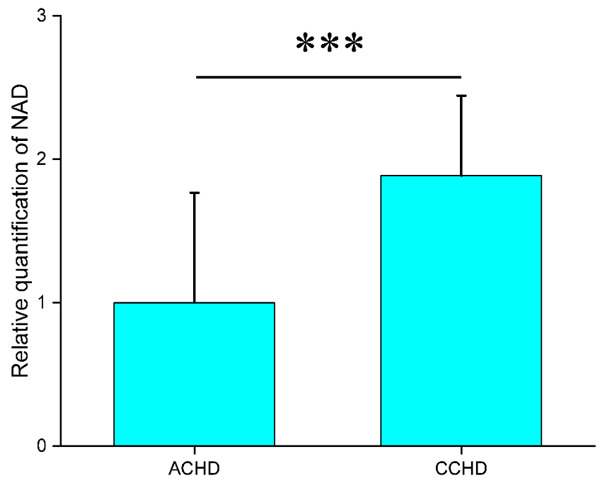
Results: A total of 71 (63%) metabolites from 113 detected substances in cardiac tissue differed between the CCHD and ACHD groups. A partial least squares discriminant analysis showed separation between the CCHD and ACHD groups. A pathway enrichment analysis revealed that the most enriched metabolic pathways were amino acid metabolism and energy metabolism. Eleven amino acids were increased in CCHD patients, indicating that protein synthesis was down-regulated. Most of the metabolites in Krebs circle were increased in CCHD patients, suggesting down regulation of aerobic energy metabolism. Hierarchical cluster analysis showed that nicotinamide adenine dinucleotide (NAD) was clustered with Krebs cycle related substrates and its level was significantly higher in CCHD than that in ACHD patients. These analyses suggest that NAD might play an important role in response to hypoxia in CCHD patients.
Conclusion: Our data showed a significantly different metabolic profile in CCHD patients compared to ACHD patients, including reduced protein synthesis and aerobic energy production, and the increased level of NAD in the myocardium may be a response mechanism to hypoxia.
Keywords: Congenital heart disease; Krebs cycle; chronic hypoxia; metabolomics; nicotinamide adenine dinucleotide.
AJTR Copyright © 2021.
Conflict of interest statement
None.
Figures

Similar articles
-
Suppression of Myocardial Hypoxia-Inducible Factor-1α Compromises Metabolic Adaptation and Impairs Cardiac Function in Patients With Cyanotic Congenital Heart Disease During Puberty.Circulation. 2021 Jun 8;143(23):2254-2272. doi: 10.1161/CIRCULATIONAHA.120.051937. Epub 2021 Mar 5. Circulation. 2021. PMID: 33663226
-
Neurodevelopmental assessment of children with congenital heart diseases using Trivandrum developmental screening chart.J Neurosci Rural Pract. 2023 Oct-Dec;14(4):692-697. doi: 10.25259/JNRP_46_2023. Epub 2023 Aug 12. J Neurosci Rural Pract. 2023. PMID: 38059228 Free PMC article.
-
Polymorphonuclear leukocyte functions in children with cyanotic and acyanotic congenital heart disease.Indian Pediatr. 1993 Jul;30(7):883-90. Indian Pediatr. 1993. PMID: 8132280
-
Catecholamine-Secreting Tumors in Pediatric Patients With Cyanotic Congenital Heart Disease.J Endocr Soc. 2019 Sep 5;3(11):2135-2150. doi: 10.1210/js.2019-00226. eCollection 2019 Nov 1. J Endocr Soc. 2019. PMID: 31687640 Free PMC article. Review.
-
Elevated serum levels of ghrelin and TNF-α in patients with cyanotic and acyanotic congenital heart disease.World J Pediatr. 2017 Apr;13(2):122-128. doi: 10.1007/s12519-016-0068-0. Epub 2016 Nov 15. World J Pediatr. 2017. PMID: 27878778 Review.
Cited by
-
Optimal Nutrition Parameters for Neonates and Infants with Congenital Heart Disease.Nutrients. 2022 Apr 17;14(8):1671. doi: 10.3390/nu14081671. Nutrients. 2022. PMID: 35458233 Free PMC article. Review.
-
Transcriptomics integrated with metabolomics reveals partial molecular mechanisms of nutritional risk and neurodevelopment in children with congenital heart disease.Front Cardiovasc Med. 2024 Aug 9;11:1414089. doi: 10.3389/fcvm.2024.1414089. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39185136 Free PMC article.
-
Metabolomics: A New Tool in Our Understanding of Congenital Heart Disease.Children (Basel). 2022 Nov 24;9(12):1803. doi: 10.3390/children9121803. Children (Basel). 2022. PMID: 36553246 Free PMC article. Review.
-
Adapting to a new environment: postnatal maturation of the human cardiomyocyte.J Physiol. 2023 Jul;601(13):2593-2619. doi: 10.1113/JP283792. Epub 2023 Apr 9. J Physiol. 2023. PMID: 37031380 Free PMC article. Review.
-
SOX7 loss-of-function variation as a cause of familial congenital heart disease.Am J Transl Res. 2022 Mar 15;14(3):1672-1684. eCollection 2022. Am J Transl Res. 2022. PMID: 35422912 Free PMC article.
References
-
- van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, Roos-Hesselink JW. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011;58:2241–7. - PubMed
-
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–900. - PubMed
-
- Bernier PL, Stefanescu A, Samoukovic G, Tchervenkov CI. The challenge of congenital heart disease worldwide: epidemiologic and demographic facts. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2010;13:26–34. - PubMed
-
- Jorgensen M, McPherson E, Zaleski C, Shivaram P, Cold C. Stillbirth: the heart of the matter. Am J Med Genet A. 2014;164A:691–9. - PubMed
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012;125:e2–e220. - PMC - PubMed
LinkOut - more resources
Full Text Sources