

Renal effects of growth hormone in health and in kidney disease
- PMID: 34143299
- PMCID: PMC8260426
- DOI: 10.1007/s00467-021-05097-6
Renal effects of growth hormone in health and in kidney disease
Abstract
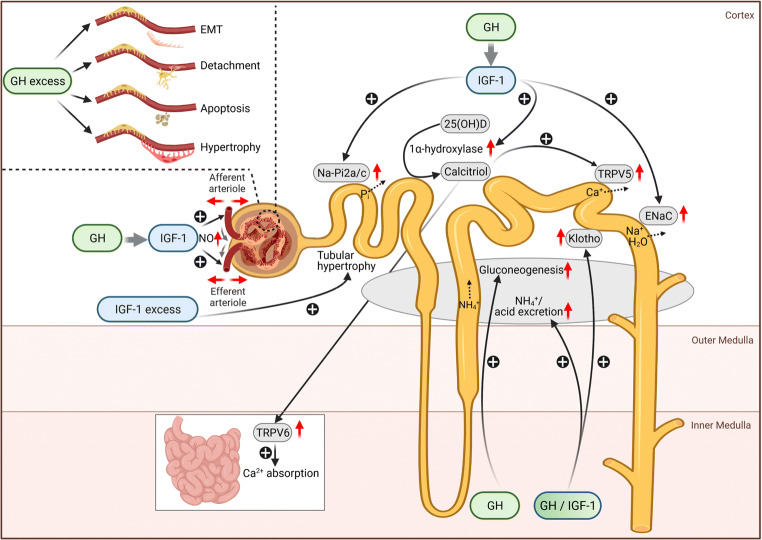
Growth hormone (GH) and its mediator insulin-like growth factor-1 (IGF-1) have manifold effects on the kidneys. GH and IGF receptors are abundantly expressed in the kidney, including the glomerular and tubular cells. GH can act either directly on the kidneys or via circulating or paracrine-synthesized IGF-1. The GH/IGF-1 system regulates glomerular hemodynamics, renal gluconeogenesis, tubular sodium and water, phosphate, and calcium handling, as well as renal synthesis of 1,25 (OH)2 vitamin D3 and the antiaging hormone Klotho. The latter also acts as a coreceptor of the phosphaturic hormone fibroblast-growth factor 23 in the proximal tubule. Recombinant human GH (rhGH) is widely used in the treatment of short stature in children, including those with chronic kidney disease (CKD). Animal studies and observations in acromegalic patients demonstrate that GH-excess can have deleterious effects on kidney health, including glomerular hyperfiltration, renal hypertrophy, and glomerulosclerosis. In addition, elevated GH in patients with poorly controlled type 1 diabetes mellitus was thought to induce podocyte injury and thereby contribute to the development of diabetic nephropathy. This manuscript gives an overview of the physiological actions of GH/IGF-1 on the kidneys and the multiple alterations of the GH/IGF-1 system and its consequences in patients with acromegaly, CKD, nephrotic syndrome, and type 1 diabetes mellitus. Finally, the impact of short- and long-term treatment with rhGH/rhIGF-1 on kidney function in patients with kidney diseases will be discussed.
Keywords: Children; Chronic kidney disease; Diabetic nephropathy; Growth hormone; Hypertrophy; IGF-1; Klotho; Nephrotic syndrome.
Figures
Similar articles
-
Growth Hormone and IGF1 Actions in Kidney Development and Function.Cells. 2021 Nov 30;10(12):3371. doi: 10.3390/cells10123371. Cells. 2021. PMID: 34943879 Free PMC article. Review.
-
Growth hormone, the insulin-like growth factor system, and the kidney.Endocr Rev. 1996 Oct;17(5):423-80. doi: 10.1210/edrv-17-5-423. Endocr Rev. 1996. PMID: 8897021 Review.
-
Influence of growth hormone and insulin-like growth factor-I on kidney function and kidney growth.Pediatr Nephrol. 1991 Jul;5(4):509-12. doi: 10.1007/BF01453692. Pediatr Nephrol. 1991. PMID: 1911130 Review.
-
Growth hormone, insulin-like growth factor-1, and the kidney: pathophysiological and clinical implications.Endocr Rev. 2014 Apr;35(2):234-81. doi: 10.1210/er.2013-1071. Epub 2013 Dec 20. Endocr Rev. 2014. PMID: 24423979 Review.
-
Mecasermin (recombinant human insulin-like growth factor I).Adv Ther. 2009 Jan;26(1):40-54. doi: 10.1007/s12325-008-0136-5. Epub 2009 Jan 28. Adv Ther. 2009. PMID: 19198769 Review.
Cited by
-
Correlation between bilateral GFR in patients with localized renal cancer after partial nephrectomy.Int Urol Nephrol. 2024 May;56(5):1617-1625. doi: 10.1007/s11255-023-03901-w. Epub 2023 Dec 23. Int Urol Nephrol. 2024. PMID: 38141102
-
Marked reduction of proteinuria after removal of a growth hormone-producing pituitary adenoma in a patient with focal segmental glomerulosclerosis: a case report and literature review.CEN Case Rep. 2023 May;12(2):164-170. doi: 10.1007/s13730-022-00739-6. Epub 2022 Oct 6. CEN Case Rep. 2023. PMID: 36201148 Free PMC article. Review.
-
Reporting a novel growth hormone receptor gene variant in an Iranian consanguineous pedigree with Laron syndrome: a case report.BMC Endocr Disord. 2023 Jul 20;23(1):155. doi: 10.1186/s12902-023-01388-1. BMC Endocr Disord. 2023. PMID: 37474955 Free PMC article.
-
Dilated cardiomyopathy in a cat with congenital hyposomatotropism.JFMS Open Rep. 2022 Mar 30;8(1):20551169221086437. doi: 10.1177/20551169221086437. eCollection 2022 Jan-Jun. JFMS Open Rep. 2022. PMID: 35368737 Free PMC article.
-
Growth Hormone and IGF1 Actions in Kidney Development and Function.Cells. 2021 Nov 30;10(12):3371. doi: 10.3390/cells10123371. Cells. 2021. PMID: 34943879 Free PMC article. Review.
References
-
- Kamenický P, Mazziotti G, Lombès M, Giustina A, Chanson P. Growth hormone, insulin-like growth factor-1, and the kidney: pathophysiological and clinical implications. Endocr Rev. 2014;35:234–281. - PubMed
-
- Feld S, Hirschberg R. Growth hormone, the insulin-like growth factor system, and the kidney. Endocr Rev. 1996;17:423–480. - PubMed
-
- Hammerman MR. The growth hormone-insulin-like growth factor axis in kidney re-revisited. Nephrol Dial Transplant. 1999;14:1853–1860. - PubMed
-
- Ogle GD, Rosenberg AR, Kainer G. Renal effects of growth hormone. I. Renal function and kidney growth. Pediatr Nephrol. 1992;6:394–398. - PubMed
-
- Ogle GD, Rosenberg AR, Kainer G. Renal effects of growth hormone. II. Electrolyte homeostasis and body composition. Pediatr Nephrol. 1992;6:483–489. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
