

Associations between Hypertriglyceridemia and Circulating Neutrophil Subpopulation in Patients with Dyslipidemia
- PMID: 34136120
- PMCID: PMC8175187
- DOI: 10.1155/2021/6695468
Associations between Hypertriglyceridemia and Circulating Neutrophil Subpopulation in Patients with Dyslipidemia
Abstract
Background: There is strong evidence to suggest that the negative influence of triglyceride-rich lipoproteins (TRLs) on atherosclerosis development and progression is at least partially mediated by their proinflammatory effects. However, the effect of hypertriglyceridemia (HTG) on the subpopulation composition of circulating neutrophils has not been studied so far. The aim of this study was to examine correlations between the level of triglycerides (TGs) and the subpopulation composition of circulating neutrophils in middle-aged patients with dyslipidemia without established atherosclerotic cardiovascular diseases (ASCVDs).
Methods: Ninety-one patients with dyslipidemia, including 22 (24.2%) patients with HTG, were enrolled in the study. Phenotying of neutrophil subpopulations was performed through flow cytometry (Navios 6/2, Beckman Coulter, USA). For phenotyping of neutrophil subpopulations, conjugated monoclonal antibodies were used: CD16, PE-Cyanine7 (Invitrogen, USA); CD11b-FITC (Beckman Coulter, USA); CD62L-PE (Beckman Coulter, USA); and CD184 (CXCR4)-PE-CF594 (BD Biosciences, USA).
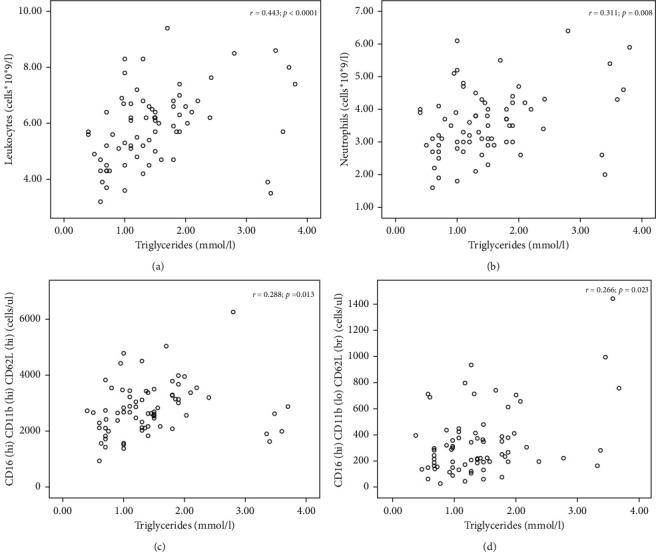
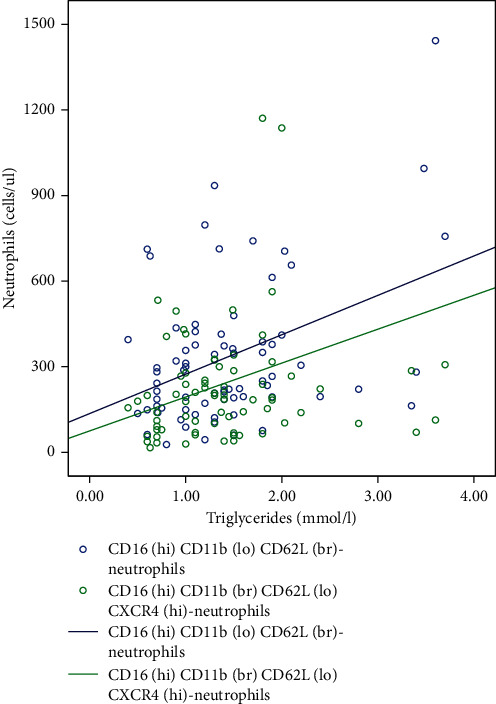
Results: Following the correlation analysis, the TG level directly correlated with the number of circulating leukocytes (r = 0.443; p < 0.0001) and neutrophils (r = 0.311; p=0.008). HTG patients displayed a significantly high number of circulating neutrophils with CD16hiCD11bhiCD62Lhi and CD16hiCD11bloCD62Lbr phenotypes. TG levels directly correlated with the number of circulating neutrophils having CD16hiCD11bhiCD62Lhi and CD16hiCD11bloCD62Lbr phenotypes. Following the linear regression analysis, statistically significant correlations between TG levels and neutrophil subpopulations having CD16hiCD11bloCD62Lbr and CD16hiCD11bbrCD62LloCXCR4hi phenotypes were established. Changes in TG levels could explain up to 19.1% of the variability in the number of studied neutrophil subpopulations.
Conclusion: Among middle-aged patients without established ASCVDs, patients with HTG demonstrated a significantly higher overall number of neutrophils and neutrophils having CD16hiCD11bhiCD62Lhi (mature neutrophils) and CD16hiCD11bloCD62Lbr (immunosuppressive neutrophils) than patients with normal TG levels. The TG level was associated with an increase in the number of CD16hiCD11bloCD62Lbr and CD16hiCD11bbrCD62LloCXCR4hi (ageing neutrophils) neutrophils, adjusted for the sex and age of the patients.
Copyright © 2021 Vadim Genkel et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Figures

Similar articles
-
Circulating Ageing Neutrophils as a Marker of Asymptomatic Polyvascular Atherosclerosis in Statin-Naïve Patients without Established Cardiovascular Disease.Int J Mol Sci. 2022 Sep 5;23(17):10195. doi: 10.3390/ijms231710195. Int J Mol Sci. 2022. PMID: 36077592 Free PMC article.
-
Associations between Circulating VEGFR2hi-Neutrophils and Carotid Plaque Burden in Patients Aged 40-64 without Established Atherosclerotic Cardiovascular Disease.J Immunol Res. 2022 Apr 26;2022:1539935. doi: 10.1155/2022/1539935. eCollection 2022. J Immunol Res. 2022. PMID: 35518568 Free PMC article.
-
[Phenotype and function of neutrophils in normal human peripheral blood].Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 2024 Oct;40(10):865-871. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 2024. PMID: 39442984 Chinese.
-
NET-producing CD16high CD62Ldim neutrophils migrate to tumor sites and predict improved survival in patients with HNSCC.Int J Cancer. 2017 Jun 1;140(11):2557-2567. doi: 10.1002/ijc.30671. Epub 2017 Mar 11. Int J Cancer. 2017. PMID: 28247912
-
Campylobacter jejuni induces differentiation of human neutrophils to the CD16hi /CD62Llo subtype.J Leukoc Biol. 2022 Dec;112(6):1457-1470. doi: 10.1002/JLB.4A0322-155RR. Epub 2022 Jul 22. J Leukoc Biol. 2022. PMID: 35866361
Cited by
-
Investigation of Lymphocyte Subsets in Peripheral Blood of Patients with Dyslipidemia.Int J Gen Med. 2021 Sep 14;14:5573-5579. doi: 10.2147/IJGM.S326628. eCollection 2021. Int J Gen Med. 2021. PMID: 34548808 Free PMC article.
-
Circulating Ageing Neutrophils as a Marker of Asymptomatic Polyvascular Atherosclerosis in Statin-Naïve Patients without Established Cardiovascular Disease.Int J Mol Sci. 2022 Sep 5;23(17):10195. doi: 10.3390/ijms231710195. Int J Mol Sci. 2022. PMID: 36077592 Free PMC article.
-
Immune-Enhancing Treatment among Acute Necrotizing Pancreatitis Patients with Metabolic Abnormalities: A Post Hoc Analysis of a Randomized Clinical Trial.Gut Liver. 2024 Sep 15;18(5):906-914. doi: 10.5009/gnl230326. Epub 2024 Feb 15. Gut Liver. 2024. PMID: 38356344 Free PMC article. Clinical Trial.
-
Bioinformatic Analyses of Peripheral Blood Transcriptome Identify Altered Neutrophil-Related Pathway and Different Transcriptomic Profiles for Acute Pancreatitis in Patients with and without Chylomicronemia Syndrome.Biomolecules. 2023 Feb 2;13(2):284. doi: 10.3390/biom13020284. Biomolecules. 2023. PMID: 36830652 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
