

An appraisal of respiratory system compliance in mechanically ventilated covid-19 patients
- PMID: 34108029
- PMCID: PMC8188162
- DOI: 10.1186/s13054-021-03518-4
An appraisal of respiratory system compliance in mechanically ventilated covid-19 patients
Abstract
Background: Heterogeneous respiratory system static compliance (CRS) values and levels of hypoxemia in patients with novel coronavirus disease (COVID-19) requiring mechanical ventilation have been reported in previous small-case series or studies conducted at a national level.
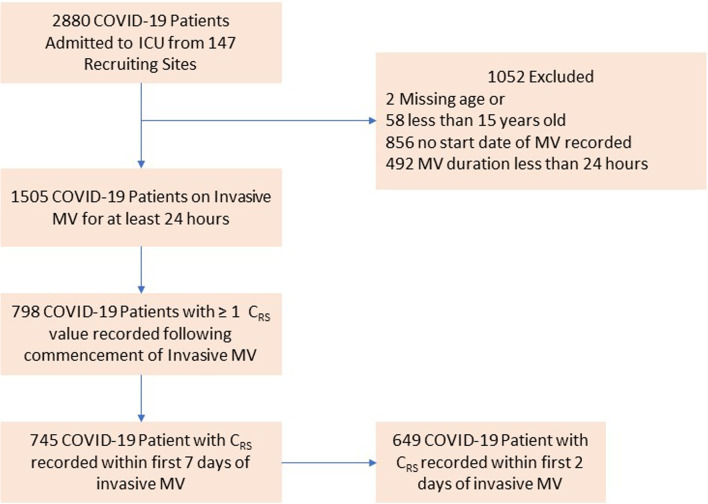
Methods: We designed a retrospective observational cohort study with rapid data gathering from the international COVID-19 Critical Care Consortium study to comprehensively describe CRS-calculated as: tidal volume/[airway plateau pressure-positive end-expiratory pressure (PEEP)]-and its association with ventilatory management and outcomes of COVID-19 patients on mechanical ventilation (MV), admitted to intensive care units (ICU) worldwide.
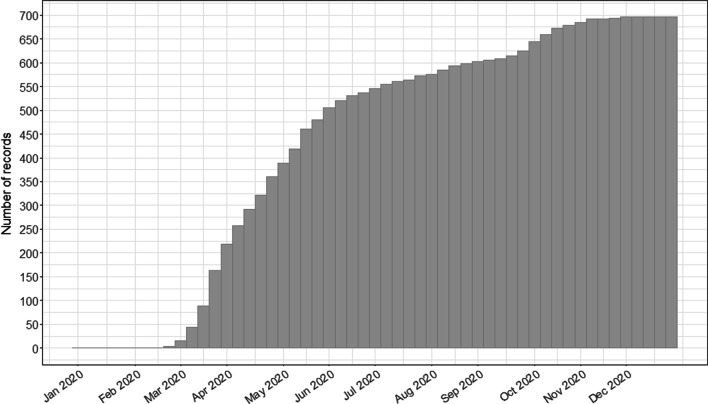
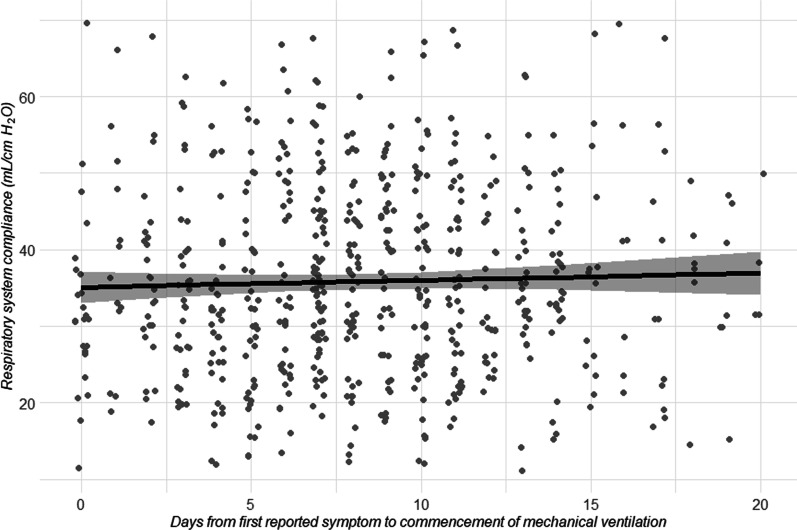
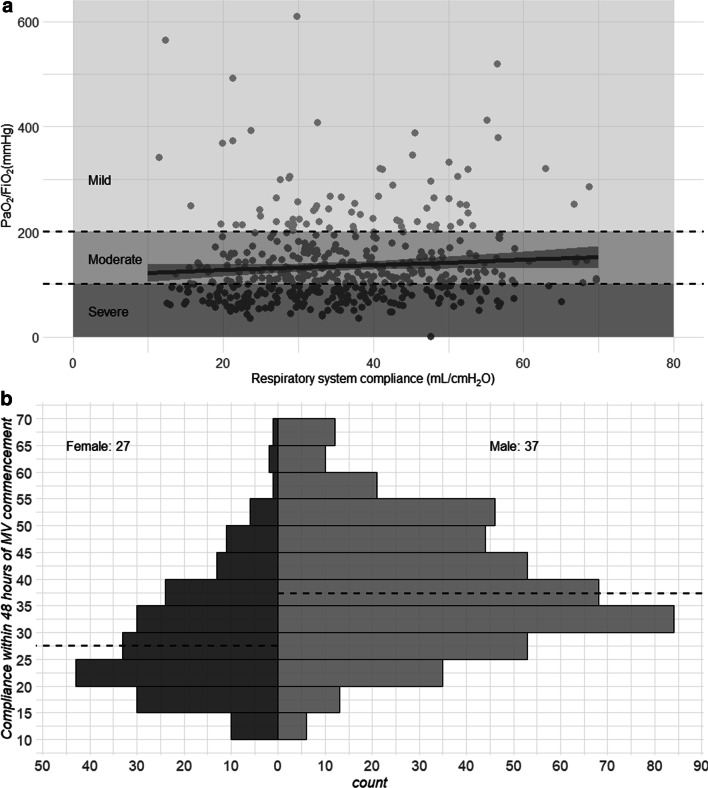
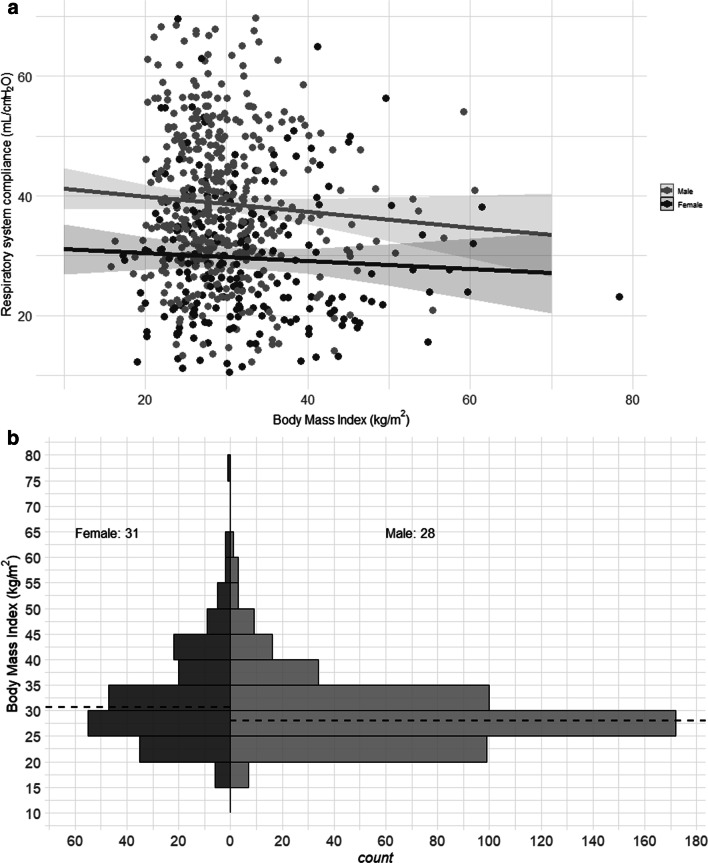
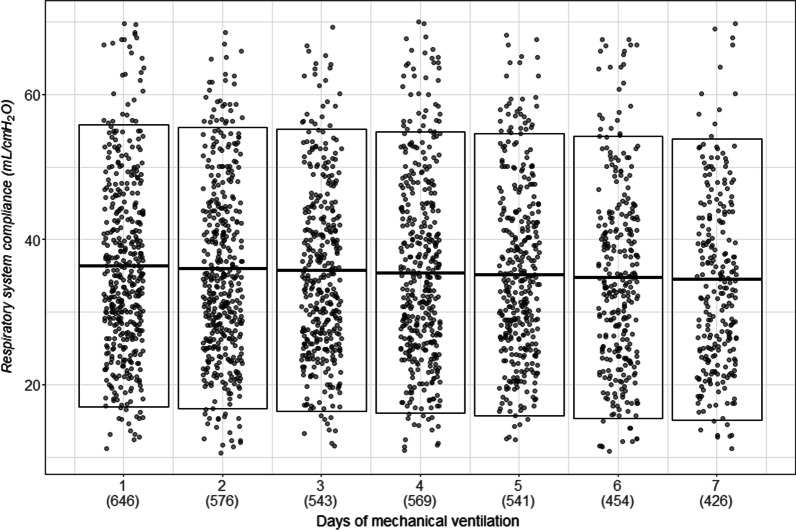
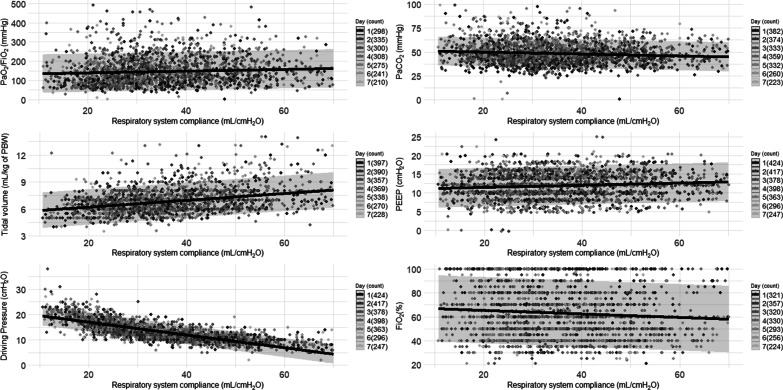
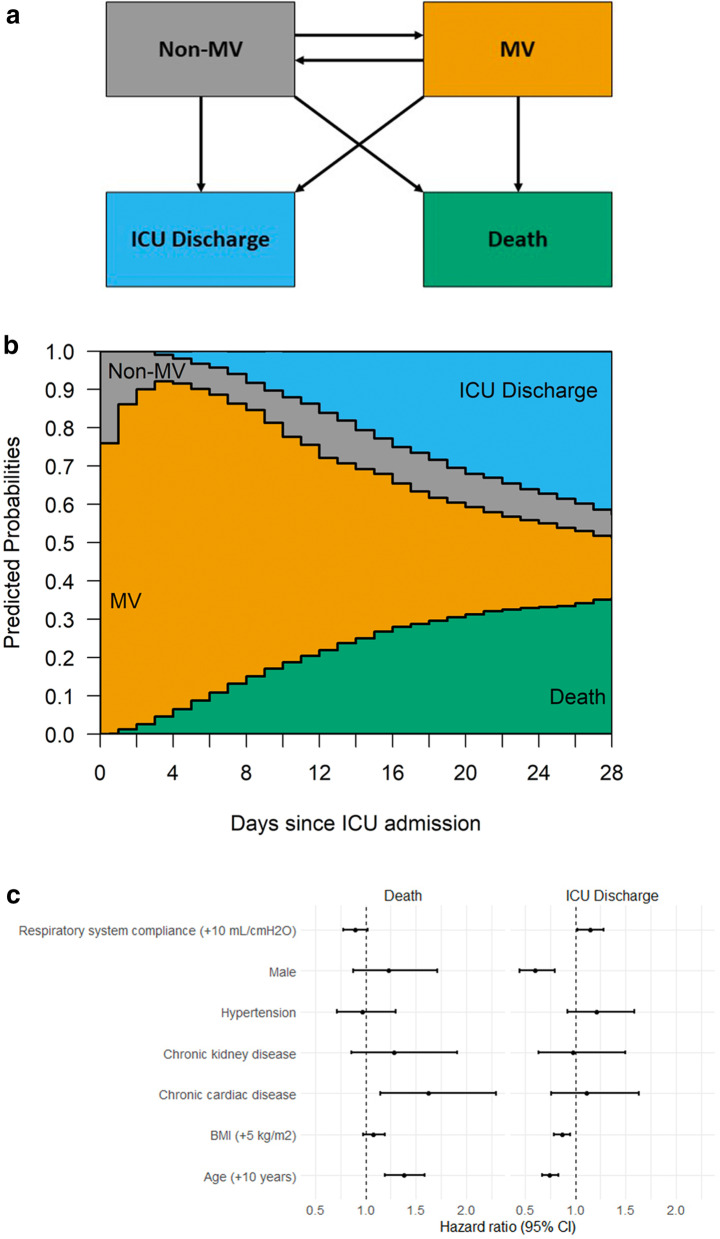
Results: We studied 745 patients from 22 countries, who required admission to the ICU and MV from January 14 to December 31, 2020, and presented at least one value of CRS within the first seven days of MV. Median (IQR) age was 62 (52-71), patients were predominantly males (68%) and from Europe/North and South America (88%). CRS, within 48 h from endotracheal intubation, was available in 649 patients and was neither associated with the duration from onset of symptoms to commencement of MV (p = 0.417) nor with PaO2/FiO2 (p = 0.100). Females presented lower CRS than males (95% CI of CRS difference between females-males: - 11.8 to - 7.4 mL/cmH2O p < 0.001), and although females presented higher body mass index (BMI), association of BMI with CRS was marginal (p = 0.139). Ventilatory management varied across CRS range, resulting in a significant association between CRS and driving pressure (estimated decrease - 0.31 cmH2O/L per mL/cmH20 of CRS, 95% CI - 0.48 to - 0.14, p < 0.001). Overall, 28-day ICU mortality, accounting for the competing risk of being discharged within the period, was 35.6% (SE 1.7). Cox proportional hazard analysis demonstrated that CRS (+ 10 mL/cm H2O) was only associated with being discharge from the ICU within 28 days (HR 1.14, 95% CI 1.02-1.28, p = 0.018).
Conclusions: This multicentre report provides a comprehensive account of CRS in COVID-19 patients on MV. CRS measured within 48 h from commencement of MV has marginal predictive value for 28-day mortality, but was associated with being discharged from ICU within the same period. Trial documentation: Available at https://www.covid-critical.com/study .
Trial registration: ACTRN12620000421932.
Keywords: ARDS; COVID-19; Compliance; Mechanical ventilation; SARS-CoV-2.
Conflict of interest statement
GLB and JF received research funds, through their affiliated institution from Fisher & Paykel. All remaining authors do not have any conflict of interest related to this report.
Figures

Similar articles
-
Clinical characteristics and outcomes of invasively ventilated patients with COVID-19 in Argentina (SATICOVID): a prospective, multicentre cohort study.Lancet Respir Med. 2021 Sep;9(9):989-998. doi: 10.1016/S2213-2600(21)00229-0. Epub 2021 Jul 2. Lancet Respir Med. 2021. PMID: 34224674 Free PMC article.
-
Longitudinal changes in compliance, oxygenation and ventilatory ratio in COVID-19 versus non-COVID-19 pulmonary acute respiratory distress syndrome.Crit Care. 2021 Jul 15;25(1):248. doi: 10.1186/s13054-021-03665-8. Crit Care. 2021. PMID: 34266454 Free PMC article.
-
Potential for the lung recruitment and the risk of lung overdistension during 21 days of mechanical ventilation in patients with COVID-19 after noninvasive ventilation failure: the COVID-VENT observational trial.BMC Anesthesiol. 2022 Mar 4;22(1):59. doi: 10.1186/s12871-022-01600-0. BMC Anesthesiol. 2022. PMID: 35246024 Free PMC article.
-
Effect of prone positioning on oxygenation and static respiratory system compliance in COVID-19 ARDS vs. non-COVID ARDS.Respir Res. 2021 Aug 6;22(1):220. doi: 10.1186/s12931-021-01819-4. Respir Res. 2021. PMID: 34362368 Free PMC article. Review.
-
Respiratory system mechanics, gas exchange, and outcomes in mechanically ventilated patients with COVID-19-related acute respiratory distress syndrome: a systematic review and meta-analysis.Lancet Respir Med. 2022 Dec;10(12):1178-1188. doi: 10.1016/S2213-2600(22)00393-9. Epub 2022 Nov 3. Lancet Respir Med. 2022. PMID: 36335956 Free PMC article. Review.
Cited by
-
Positive end-expiratory pressure induced changes in airway driving pressure in mechanically ventilated COVID-19 Acute Respiratory Distress Syndrome patients.Crit Care. 2023 Mar 21;27(1):118. doi: 10.1186/s13054-023-04345-5. Crit Care. 2023. PMID: 36945013 Free PMC article.
-
The Effect of Oxygenation Impairment and Compliance on Mortality Among Subjects With COVID-19 Requiring Mechanical Ventilation.Respir Care. 2023 Nov;68(11):1565-1568. doi: 10.4187/respcare.10776. Epub 2023 Jun 6. Respir Care. 2023. PMID: 37280073 Free PMC article. No abstract available.
-
Non-Invasive Multimodal Neuromonitoring in Non-Critically Ill Hospitalized Adult Patients With COVID-19: A Systematic Review and Meta-Analysis.Front Neurol. 2022 Apr 14;13:814405. doi: 10.3389/fneur.2022.814405. eCollection 2022. Front Neurol. 2022. PMID: 35493827 Free PMC article.
-
Brazilian initial experience with lung transplantation due to irreversible lung fibrosis post-COVID-19 in a national reference center: a cohort study.Sao Paulo Med J. 2021 Dec 17;140(1):153-9. doi: 10.1590/1516-3180.2021.0842.R1.13102021. Online ahead of print. Sao Paulo Med J. 2021. PMID: 34932782 Free PMC article.
-
Respiratory mechanics in late COVID-19 ARDS - a restrictive pattern is strongly associated with death. A cohort study.Anaesthesiol Intensive Ther. 2022;54(4):295-301. doi: 10.5114/ait.2022.121091. Anaesthesiol Intensive Ther. 2022. PMID: 36458666 Free PMC article.
References
-
- Karagiannidis C, Mostert C, Hentschker C, Voshaar T, Malzahn J, Schillinger G, et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: an observational study. Lancet Respir Med [Internet]. Elsevier; 2020 [cited 2020 Aug 6];0. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2213260020303167. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
