

Relationship between ventilator-associated pneumonia and mortality in COVID-19 patients: a planned ancillary analysis of the coVAPid cohort
- PMID: 34034777
- PMCID: PMC8146175
- DOI: 10.1186/s13054-021-03588-4
Relationship between ventilator-associated pneumonia and mortality in COVID-19 patients: a planned ancillary analysis of the coVAPid cohort
Erratum in
-
Correction to: Relationship between ventilator-associated pneumonia and mortality in COVID-19 patients: a planned ancillary analysis of the coVAPid cohort.Crit Care. 2021 Aug 9;25(1):284. doi: 10.1186/s13054-021-03713-3. Crit Care. 2021. PMID: 34372897 Free PMC article. No abstract available.
Abstract
Background: Patients with SARS-CoV-2 infection are at higher risk for ventilator-associated pneumonia (VAP). No study has evaluated the relationship between VAP and mortality in this population, or compared this relationship between SARS-CoV-2 patients and other populations. The main objective of our study was to determine the relationship between VAP and mortality in SARS-CoV-2 patients.
Methods: Planned ancillary analysis of a multicenter retrospective European cohort. VAP was diagnosed using clinical, radiological and quantitative microbiological criteria. Univariable and multivariable marginal Cox's regression models, with cause-specific hazard for duration of mechanical ventilation and ICU stay, were used to compare outcomes between study groups. Extubation, and ICU discharge alive were considered as events of interest, and mortality as competing event.
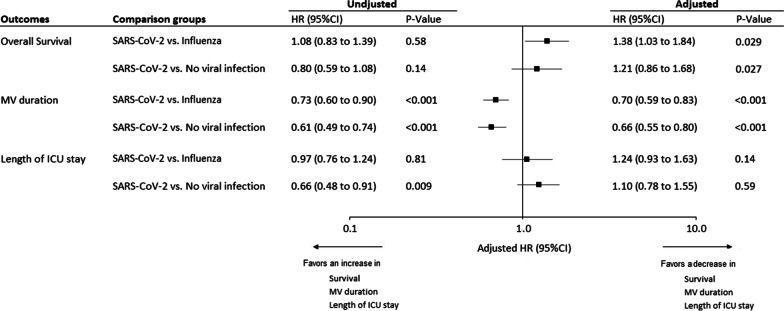
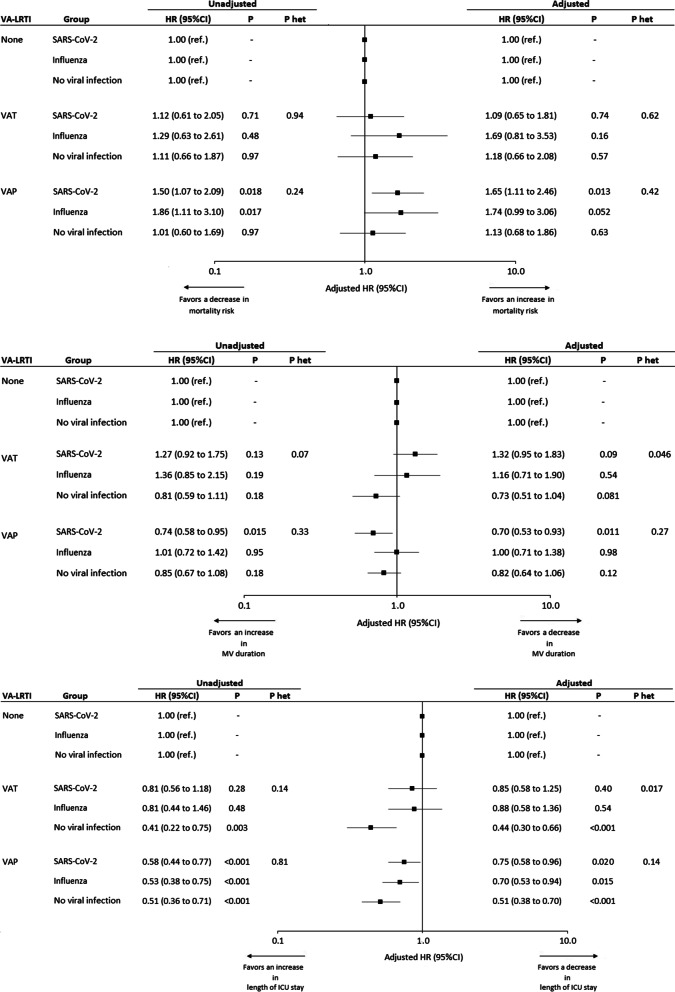
Findings: Of 1576 included patients, 568 were SARS-CoV-2 pneumonia, 482 influenza pneumonia, and 526 no evidence of viral infection at ICU admission. VAP was associated with significantly higher risk for 28-day mortality in SARS-CoV-2 (adjusted HR 1.70 (95% CI 1.16-2.47), p = 0.006), and influenza groups (1.75 (1.03-3.02), p = 0.045), but not in the no viral infection group (1.07 (0.64-1.78), p = 0.79). VAP was associated with significantly longer duration of mechanical ventilation in the SARS-CoV-2 group, but not in the influenza or no viral infection groups. VAP was associated with significantly longer duration of ICU stay in the 3 study groups. No significant difference was found in heterogeneity of outcomes related to VAP between the 3 groups, suggesting that the impact of VAP on mortality was not different between study groups.
Interpretation: VAP was associated with significantly increased 28-day mortality rate in SARS-CoV-2 patients. However, SARS-CoV-2 pneumonia, as compared to influenza pneumonia or no viral infection, did not significantly modify the relationship between VAP and 28-day mortality.
Clinical trial registration: The study was registered at ClinicalTrials.gov, number NCT04359693.
Keywords: COVID-19; Mortality; Ventilator-associated pneumonia.
Conflict of interest statement
AR received personal fees from MaatPharma, IML received personal fees from MSD, and Gilead. AA received personal fees from Lilly Foundation, and grants from Grifols and Fischer & Paykel. CEL received personal fees from Bayer, Merck, Aerogen, Biomérieux, ThermoFischer Brahms, and Carmat. SN received personal fees from MSD, Bio Rad, BioMérieux, Gilead, and Pfizer. All other authors declare no competing interests.
Figures
Similar articles
-
Relationship between corticosteroid use and incidence of ventilator-associated pneumonia in COVID-19 patients: a retrospective multicenter study.Crit Care. 2022 Sep 27;26(1):292. doi: 10.1186/s13054-022-04170-2. Crit Care. 2022. PMID: 36167550 Free PMC article.
-
Hospital-Acquired Pneumonia/Ventilator-Associated Pneumonia and Ventilator-Associated Tracheobronchitis in COVID-19.Semin Respir Crit Care Med. 2022 Apr;43(2):243-247. doi: 10.1055/s-0041-1740334. Epub 2022 Jan 18. Semin Respir Crit Care Med. 2022. PMID: 35042264
-
Invasive pulmonary aspergillosis among intubated patients with SARS-CoV-2 or influenza pneumonia: a European multicenter comparative cohort study.Crit Care. 2022 Jan 4;26(1):11. doi: 10.1186/s13054-021-03874-1. Crit Care. 2022. PMID: 34983611 Free PMC article.
-
Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia.Cochrane Database Syst Rev. 2013 Aug 13;(8):CD008367. doi: 10.1002/14651858.CD008367.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2016 Oct 25;10:CD008367. doi: 10.1002/14651858.CD008367.pub3. PMID: 23939759 Updated. Review.
-
Incidence, Risk Factors, and Outcomes of Ventilator-Associated Pneumonia in Traumatic Brain Injury: A Meta-analysis.Neurocrit Care. 2020 Feb;32(1):272-285. doi: 10.1007/s12028-019-00773-w. Neurocrit Care. 2020. PMID: 31300956 Free PMC article. Review.
Cited by
-
Incidence of Carbapenem-Resistant Gram-Negative Bacterial Infections in Critically Ill Patients with COVID-19 as Compared to Non-COVID-19 Patients: A Prospective Case-Control Study.Crit Care Res Pract. 2024 Jun 22;2024:7102082. doi: 10.1155/2024/7102082. eCollection 2024. Crit Care Res Pract. 2024. PMID: 38947882 Free PMC article.
-
Tracheostomy timing and clinical outcomes in ventilated COVID-19 patients: a systematic review and meta-analysis.Crit Care. 2022 Feb 8;26(1):40. doi: 10.1186/s13054-022-03904-6. Crit Care. 2022. PMID: 35135597 Free PMC article.
-
Comparison of Ventilator-Associated Pneumonia in Patients Admitted to Intensive Care for COVID-19 Versus Other Reasons: A Single-Centered Study.Turk J Anaesthesiol Reanim. 2022 Jun;50(Supp1):S22-S28. doi: 10.5152/TJAR.2022.21310. Turk J Anaesthesiol Reanim. 2022. PMID: 35775794 Free PMC article.
-
Prevention and treatment of ventilator-associated pneumonia in COVID-19.Front Pharmacol. 2022 Oct 19;13:945892. doi: 10.3389/fphar.2022.945892. eCollection 2022. Front Pharmacol. 2022. PMID: 36339583 Free PMC article. Review.
-
COVID-19 Secondary Infections in ICU Patients and Prevention Control Measures: A Preliminary Prospective Multicenter Study.Antibiotics (Basel). 2022 Jul 28;11(8):1016. doi: 10.3390/antibiotics11081016. Antibiotics (Basel). 2022. PMID: 36009884 Free PMC article.
References
-
- Rouzé A, Martin-Loeches I, Povoa P, Makris D, Artigas A, Bouchereau M, Lambiotte F, Metzelard M, Cuchet P, Boulle Geronimi C, Labruyere M, Tamion F, Nyunga M, Luyt C-E, Labreuche J, Pouly O, Bardin J, Saade A, Asfar P, Baudel J-L, Beurton A, Garot D, Ioannidou I, Kreitmann L, Llitjos J-F, Magira E, Mégarbane B, Meguerditchian D, Moglia E, Mekontso-Dessap A, et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: a European multicenter cohort study. Intensive Care Med. 2021;47:188–98. - PMC - PubMed
-
- Maes M, Higginson E, Pereira-Dias J, Curran MD, Parmar S, Khokhar F, Cuchet-Lourenço D, Lux J, Sharma-Hajela S, Ravenhill B, Hamed I, Heales L, Mahroof R, Solderholm A, Forrest S, Sridhar S, Brown NM, Baker S, Navapurkar V, Dougan G, Bartholdson Scott J, Conway Morris A. Ventilator-associated pneumonia in critically ill patients with COVID-19. Crit Care. 2021;25:25. doi: 10.1186/s13054-021-03460-5. - DOI - PMC - PubMed
-
- Pickens CO, Gao CA, Cuttica M, Smith SB, Pesce L, Grant R, Kang M, Morales-Nebreda L, Bavishi AA, Arnold J, Pawlowski A, Qi C, Budinger GS, Singer BD, Wunderink RG, Investigators for the NC. Bacterial superinfection pneumonia in SARS-CoV-2 respiratory failure. medRxiv 2021:2021.01.12.20248588.
-
- Razazi K, Arrestier R, Haudebourg AF, Benelli B, Carteaux G, Decousser J, Fourati S, Woerther PL, Schlemmer F, Charles-Nelson A, Botterel F, de Prost N, Mekontso Dessap A. Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit Care. 2020;24:699. doi: 10.1186/s13054-020-03417-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
