

Molecular subtypes of colorectal cancer: An emerging therapeutic opportunity for personalized medicine
- PMID: 33997160
- PMCID: PMC8099693
- DOI: 10.1016/j.gendis.2019.10.013
Molecular subtypes of colorectal cancer: An emerging therapeutic opportunity for personalized medicine
Abstract
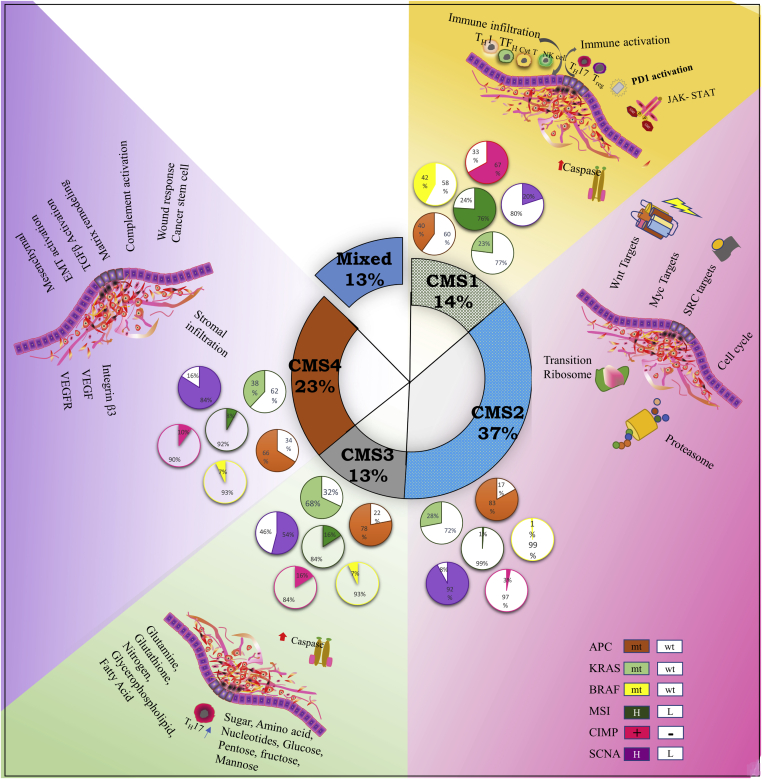
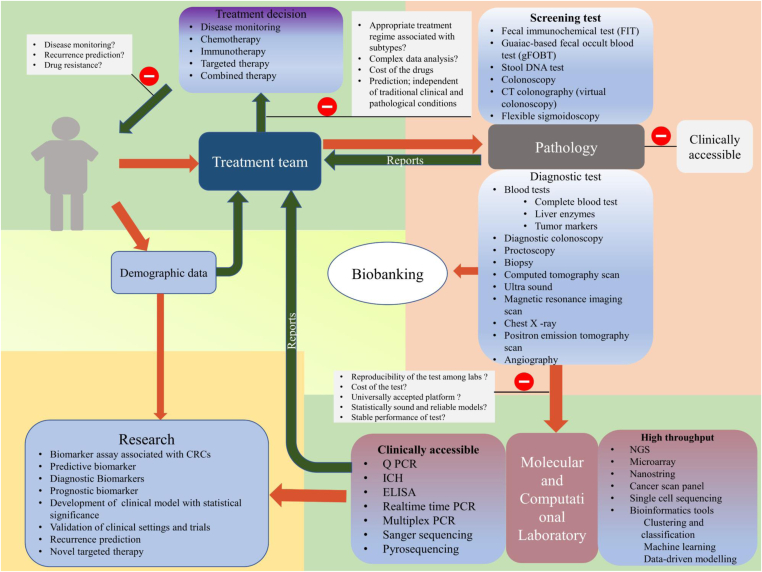
Molecular subtypes-based therapies offer new potential framework for desired and precise outcome in clinical settings. Current treatment strategies in colorectal cancer are largely 'one drug fit all' model for patients that display same pathological conditions. However, CRC is a very heterogenous set of malignancy that does not support for above criteria. Each subtype displays different pathological and genetic signatures. Based on these features, therapeutic stratification for individual patients may be designed, which may ultimately lead to improved therapeutic outcomes. In this comprehensive review, we have attempted to briefly outline major CRC pathways. A detailed overview of molecular subtypes and their clinical significance has been discussed. Present and future methods, governing CRC subtyping in the era of personalized therapy with a special emphasis on CMS subtypes of CRC has been reviewed. Together, discovery and validation of new CRC patient stratification methods, screening for novel therapeutic targets, and enhanced diagnosis of CRC may improve the treatment outcome.
Keywords: Biomarkers; CMS subtypes; Immunotherapy; Molecular screening; Personalized medicine.
© 2019 Chongqing Medical University. Production and hosting by Elsevier B.V.
Figures
Similar articles
-
Molecular subtyping in colorectal cancer: A bridge to personalized therapy (Review).Oncol Lett. 2023 Apr 18;25(6):230. doi: 10.3892/ol.2023.13816. eCollection 2023 Jun. Oncol Lett. 2023. PMID: 37153060 Free PMC article. Review.
-
Genetic Molecular Subtypes in Optimizing Personalized Therapy for Metastatic Colorectal Cancer.Curr Drug Targets. 2018;19(15):1731-1737. doi: 10.2174/1389450119666180803122744. Curr Drug Targets. 2018. PMID: 30073926 Review.
-
Molecular subtypes of colorectal cancer in the era of precision oncotherapy: Current inspirations and future challenges.Cancer Med. 2024 Jul;13(14):e70041. doi: 10.1002/cam4.70041. Cancer Med. 2024. PMID: 39054866 Free PMC article. Review.
-
The Evolving Role of Consensus Molecular Subtypes: a Step Beyond Inpatient Selection for Treatment of Colorectal Cancer.Curr Treat Options Oncol. 2021 Nov 6;22(12):113. doi: 10.1007/s11864-021-00913-5. Curr Treat Options Oncol. 2021. PMID: 34741675 Review.
-
Principles of Molecular Utility for CMS Classification in Colorectal Cancer Management.Cancers (Basel). 2023 May 13;15(10):2746. doi: 10.3390/cancers15102746. Cancers (Basel). 2023. PMID: 37345083 Free PMC article. Review.
Cited by
-
Developing a taxonomy for colorectal cancer.Elife. 2022 Nov 11;11:e84025. doi: 10.7554/eLife.84025. Elife. 2022. PMID: 36367433 Free PMC article.
-
LincROR promotes tumor growth of colorectal cancer through the miR-145/WNT2B/WNT10A/Wnt/β-catenin regulatory axis.PLoS One. 2024 Nov 15;19(11):e0312417. doi: 10.1371/journal.pone.0312417. eCollection 2024. PLoS One. 2024. PMID: 39546475 Free PMC article.
-
Biomarkers of lymph node metastasis in colorectal cancer: update.Front Oncol. 2024 Sep 12;14:1409627. doi: 10.3389/fonc.2024.1409627. eCollection 2024. Front Oncol. 2024. PMID: 39328205 Free PMC article. Review.
-
Links Between N 6-Methyladenosine and Tumor Microenvironments in Colorectal Cancer.Front Cell Dev Biol. 2022 Feb 10;10:807129. doi: 10.3389/fcell.2022.807129. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 35223837 Free PMC article.
-
Molecular subtyping in colorectal cancer: A bridge to personalized therapy (Review).Oncol Lett. 2023 Apr 18;25(6):230. doi: 10.3892/ol.2023.13816. eCollection 2023 Jun. Oncol Lett. 2023. PMID: 37153060 Free PMC article. Review.
References
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2019. CA: A Cancer J Clin. 2019;69(1):7–34. - PubMed
-
- Misale S., Di Nicolantonio F., Sartore-Bianchi A., Siena S., Bardelli A. Resistance to anti-EGFR therapy in colorectal cancer: from heterogeneity to convergent evolution. Cancer Discov. 2014;4(11):1269–1280. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
