

Development of an automated closed-loop β-blocker delivery system to stably reduce myocardial oxygen consumption without inducing circulatory collapse in a canine heart failure model: a proof of concept study
- PMID: 33969457
- PMCID: PMC9162998
- DOI: 10.1007/s10877-021-00717-w
Development of an automated closed-loop β-blocker delivery system to stably reduce myocardial oxygen consumption without inducing circulatory collapse in a canine heart failure model: a proof of concept study
Abstract
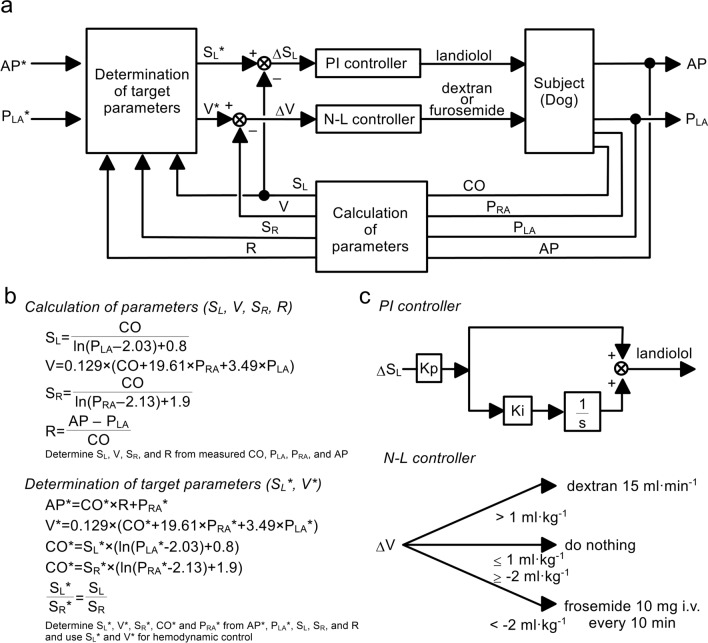
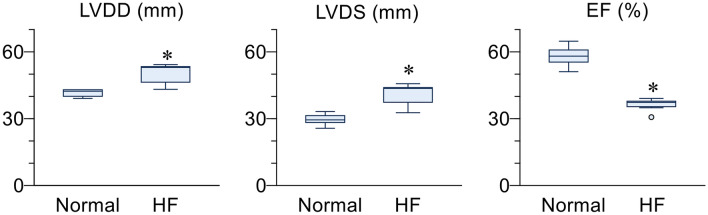
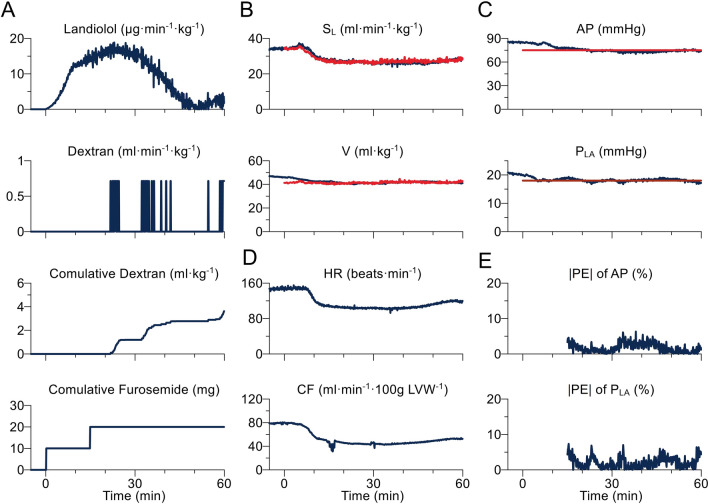
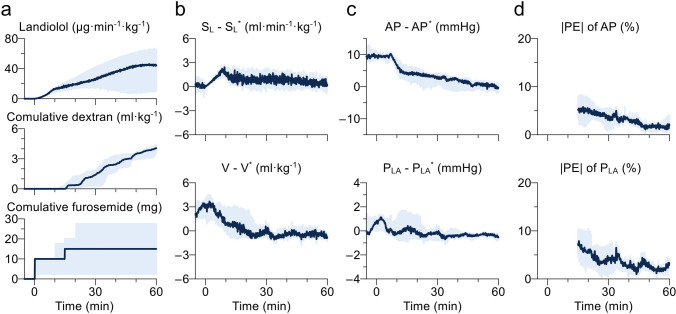
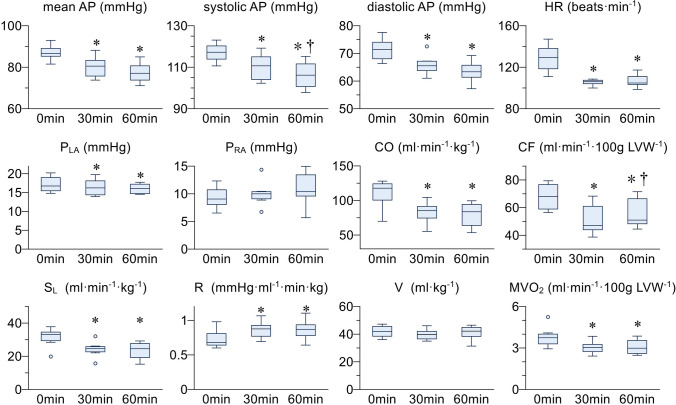
Beta-blockers are well known to reduce myocardial oxygen consumption (MVO2) and improve the prognosis of heart failure (HF) patients. However, its negative chronotropic and inotropic effects limit their use in the acute phase of HF due to the risk of circulatory collapse. In this study, as a first step for a safe β-blocker administration strategy, we aimed to develop and evaluate the feasibility of an automated β-blocker administration system. We developed a system to monitor arterial pressure (AP), left atrial pressure (PLA), right atrial pressure, and cardiac output. Using negative feedback of hemodynamics, the system controls AP and PLA by administering landiolol (an ultra-short-acting β-blocker), dextran, and furosemide. We applied the system for 60 min to 6 mongrel dogs with rapid pacing-induced HF. In all dogs, the system automatically adjusted the doses of the drugs. Mean AP and mean PLA were controlled within the acceptable ranges (AP within 5 mmHg below target; PLA within 2 mmHg above target) more than 95% of the time. Median absolute performance error was small for AP [median (interquartile range), 3.1% (2.2-3.8)] and PLA [3.6% (2.2-5.7)]. The system decreased MVO2 and PLA significantly. We demonstrated the feasibility of an automated β-blocker administration system in a canine model of acute HF. The system controlled AP and PLA to avoid circulatory collapse, and reduced MVO2 significantly. As the system can help the management of patients with HF, further validations in larger samples and development for clinical applications are warranted.
Keywords: Automated drug delivery; Beta-blocker; Closed-loop control; Hemodynamics.
© 2021. The Author(s).
Conflict of interest statement
KS received research funding from Omron Healthcare Co., Ltd., Abiomed Japan K.K., and Zeon Medical Inc., and honoraria from Abiomed Japan K.K. KU received research funding from A&D Co., Ltd.
Figures
Similar articles
-
Automated drug delivery system to control systemic arterial pressure, cardiac output, and left heart filling pressure in acute decompensated heart failure.J Appl Physiol (1985). 2006 Apr;100(4):1278-86. doi: 10.1152/japplphysiol.01206.2005. Epub 2005 Dec 22. J Appl Physiol (1985). 2006. PMID: 16373447
-
Less Invasive and Inotrope-Reduction Approach to Automated Closed-Loop Control of Hemodynamics in Decompensated Heart Failure.IEEE Trans Biomed Eng. 2016 Aug;63(8):1699-708. doi: 10.1109/TBME.2015.2499782. Epub 2015 Nov 11. IEEE Trans Biomed Eng. 2016. PMID: 26571509
-
Computer-controlled closed-loop drug infusion system for automated hemodynamic resuscitation in endotoxin-induced shock.BMC Anesthesiol. 2017 Oct 23;17(1):145. doi: 10.1186/s12871-017-0437-9. BMC Anesthesiol. 2017. PMID: 29061119 Free PMC article.
-
[Beta blockers in therapy of chronic heart failure].Herz. 2002 Mar;27(2):150-65. doi: 10.1007/s00059-002-2353-z. Herz. 2002. PMID: 12025460 Review. German.
-
[Heart rate and outcome in patients with acute and chronic heart failure].G Ital Cardiol (Rome). 2016 Mar;17(3 Suppl 1):3S-16. doi: 10.1714/2192.23678. G Ital Cardiol (Rome). 2016. PMID: 27030005 Review. Italian.
Cited by
-
Computer-controlled closed-loop norepinephrine infusion system for automated control of mean arterial pressure in dogs under isoflurane-induced hypotension: a feasibility study.Front Vet Sci. 2024 May 31;11:1374356. doi: 10.3389/fvets.2024.1374356. eCollection 2024. Front Vet Sci. 2024. PMID: 38881786 Free PMC article.
References
-
- Aurbach GD, Spiegel AM, Gardner JD. Beta-adrenergic receptors, cyclic AMP, and ion transport in the avian erythrocyte. Adv Cyclic Nucleotide Res. 1975;5:117–32. - PubMed
-
- Al-Hesayen A, Azevedo ER, Floras JS, Hollingshead S, Lopaschuk GD, Parker JD. Selective versus nonselective beta-adrenergic receptor blockade in chronic heart failure: differential effects on myocardial energy substrate utilization. Eur J Heart Fail. 2005;7:618–23. doi: 10.1016/j.ejheart.2004.04.015. - DOI - PubMed
-
- Fung JWH, Yu CM, Yip G, Chan S, Yandle TG, Richards AM, et al. Effect of beta blockade (carvedilol or metoprolol) on activation of the renin-angiotensin-aldosterone system and natriuretic peptides in chronic heart failure. Am J Cardiol. 2003;92:406–10. doi: 10.1016/S0002-9149(03)00658-1. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
