

Framework to Classify Reverse Cardiac Remodeling With Mechanical Circulatory Support: The Utah-Inova Stages
- PMID: 33947201
- PMCID: PMC8137588
- DOI: 10.1161/CIRCHEARTFAILURE.120.007991
Framework to Classify Reverse Cardiac Remodeling With Mechanical Circulatory Support: The Utah-Inova Stages
Abstract
Background: Variable definitions and an incomplete understanding of the gradient of reverse cardiac remodeling following continuous flow left ventricular assist device (LVAD) implantation has limited the field of myocardial plasticity. We evaluated the continuum of LV remodeling by serial echocardiographic imaging to define 3 stages of reverse cardiac remodeling following LVAD.
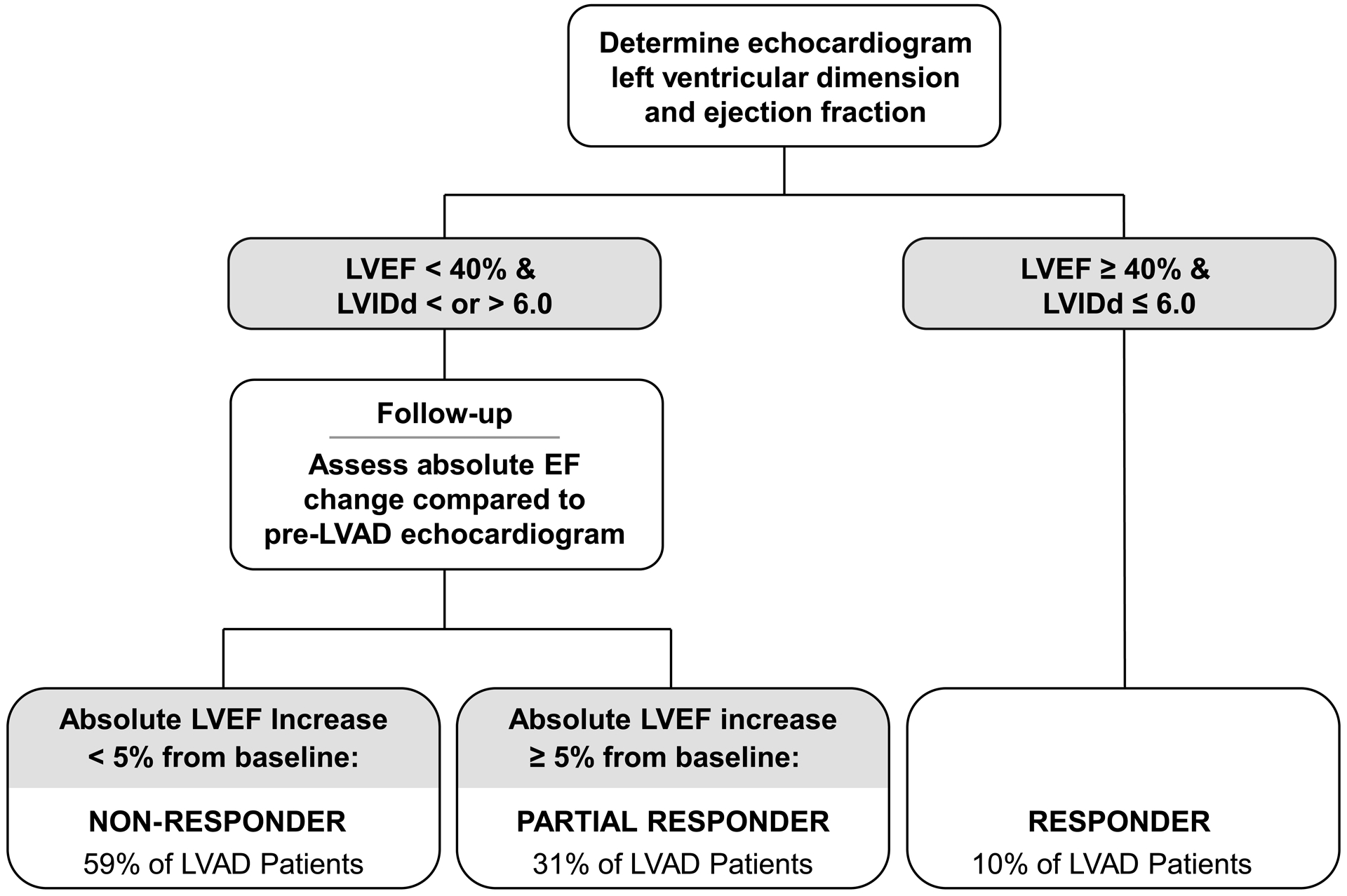
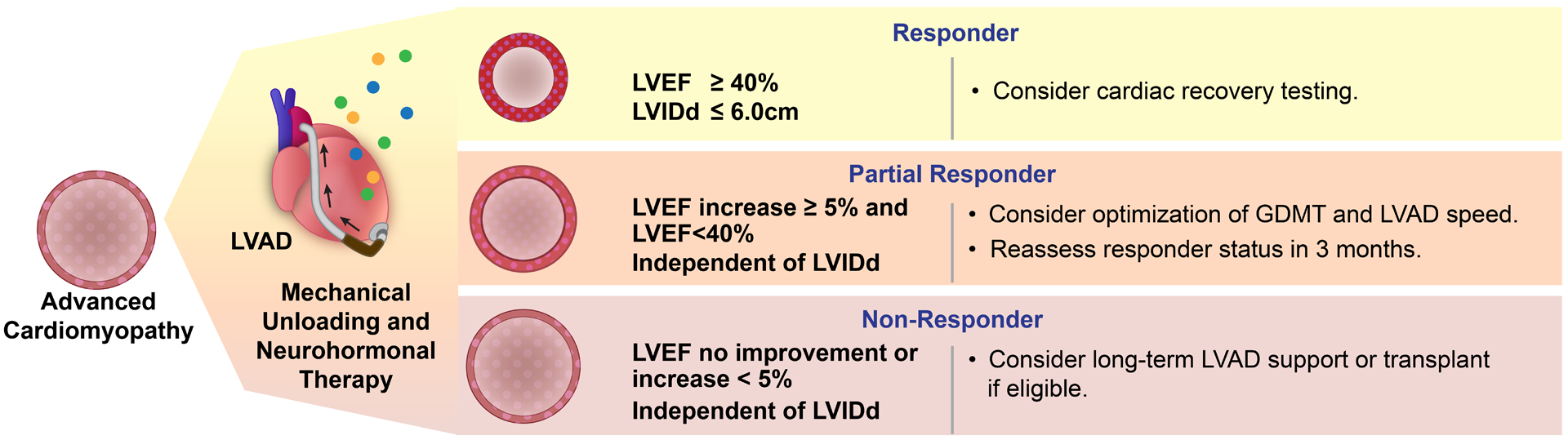
Methods: The study enrolled consecutive LVAD patients across 4 study sites. A blinded echocardiographer evaluated the degree of structural (LV internal dimension at end-diastole [LVIDd]) and functional (LV ejection fraction [LVEF]) change after LVAD. Patients experiencing an improvement in LVEF ≥40% and LVIDd ≤6.0 cm were termed responders, absolute change in LVEF of ≥5% and LVEF <40% were termed partial responders, and the remaining patients with no significant improvement in LVEF were termed nonresponders.
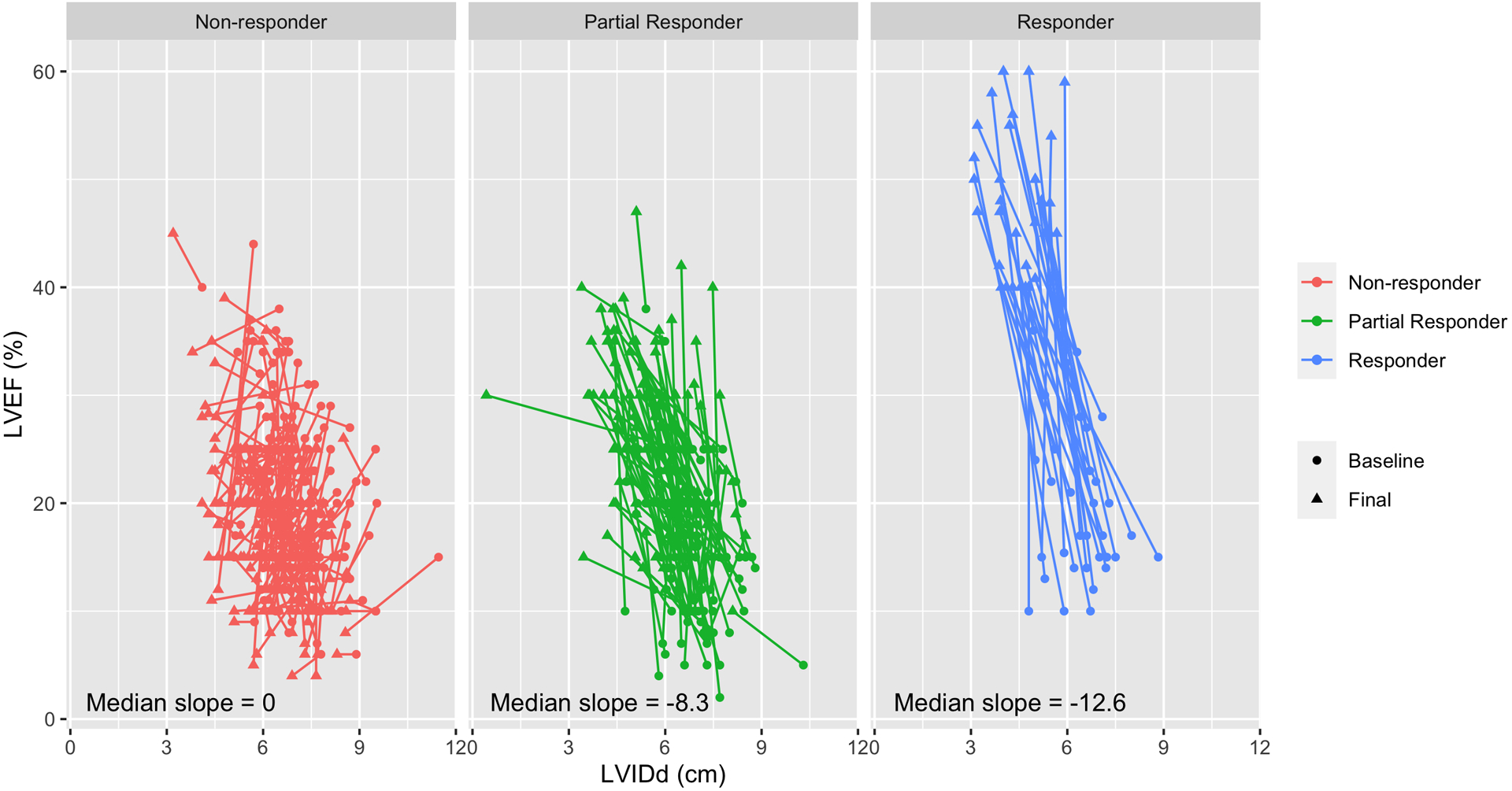
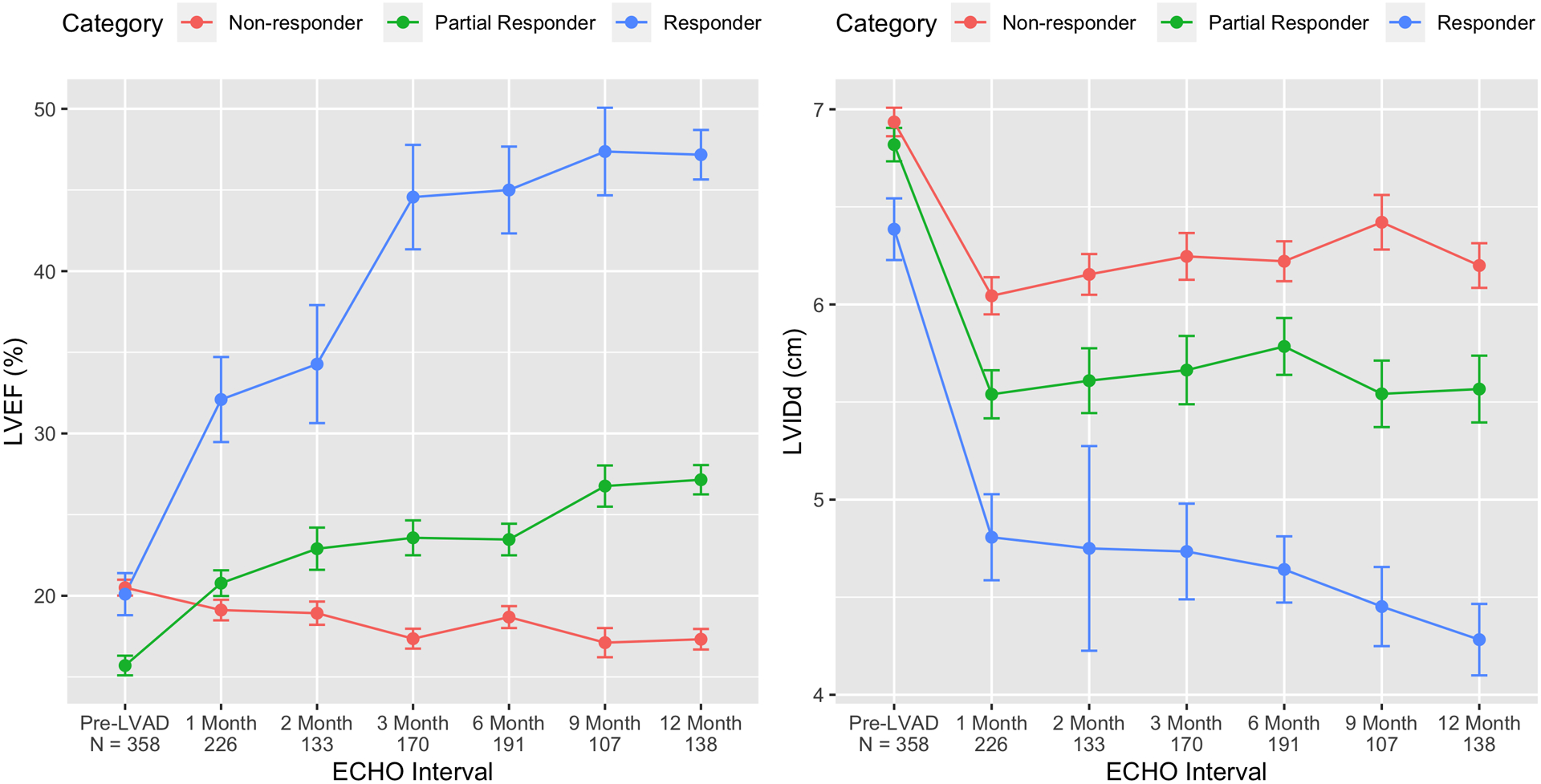
Results: Among 358 LVAD patients, 34 (10%) were responders, 112 (31%) partial responders, and the remaining 212 (59%) were nonresponders. The use of guideline-directed medical therapy for heart failure was higher in partial responders and responders. Structural changes (LVIDd) followed a different pattern with significant improvements even in patients who had minimal LVEF improvement. With mechanical unloading, the median reduction in LVIDd was -0.6 cm (interquartile range [IQR], -1.1 to -0.1 cm; nonresponders), -1.1 cm (IQR, -1.8 to -0.4 cm; partial responders), and -1.9 cm (IQR, -2.9 to -1.1 cm; responders). Similarly, the median change in LVEF was -2% (IQR, -6% to 1%), 9% (IQR, 6%-14%), and 27% (IQR, 23%-33%), respectively.
Conclusions: Reverse cardiac remodeling associated with durable LVAD support is not an all-or-none phenomenon and manifests in a continuous spectrum. Defining 3 stages across this continuum can inform clinical management, facilitate the field of myocardial plasticity, and improve the design of future investigations.
Keywords: cardiomyopathy; heart failure; left ventricular remodeling; myocardial recovery; ventricular assist device.
Figures

Similar articles
-
LVAD decommissioning for myocardial recovery: Long-term ventricular remodeling and adverse events.J Heart Lung Transplant. 2021 Dec;40(12):1560-1570. doi: 10.1016/j.healun.2021.08.001. Epub 2021 Aug 11. J Heart Lung Transplant. 2021. PMID: 34479776 Free PMC article.
-
Assessment of myocardial viability and left ventricular function in patients supported by a left ventricular assist device.J Heart Lung Transplant. 2014 Apr;33(4):372-81. doi: 10.1016/j.healun.2014.01.866. Epub 2014 Jan 27. J Heart Lung Transplant. 2014. PMID: 24582837 Free PMC article.
-
Myocardial atrophy and chronic mechanical unloading of the failing human heart: implications for cardiac assist device-induced myocardial recovery.J Am Coll Cardiol. 2014 Oct 14;64(15):1602-12. doi: 10.1016/j.jacc.2014.05.073. J Am Coll Cardiol. 2014. PMID: 25301465
-
The paradox of left ventricular assist device unloading and myocardial recovery in end-stage dilated cardiomyopathy: implications for heart failure in the elderly.Heart Fail Rev. 2012 Sep;17(4-5):615-33. doi: 10.1007/s10741-012-9300-8. Heart Fail Rev. 2012. PMID: 22258830 Review.
-
The Effect of Left Ventricular Assist Device Therapy on Cardiac Biomarkers: Implications for the Identification of Myocardial Recovery.Curr Heart Fail Rep. 2018 Aug;15(4):250-259. doi: 10.1007/s11897-018-0399-3. Curr Heart Fail Rep. 2018. PMID: 29971612 Review.
Cited by
-
Clinical myocardial recovery in advanced heart failure with long term left ventricular assist device support.J Heart Lung Transplant. 2022 Oct;41(10):1324-1334. doi: 10.1016/j.healun.2022.05.015. Epub 2022 May 28. J Heart Lung Transplant. 2022. PMID: 35835680 Free PMC article. Review.
-
Cardiac mechanics and reverse remodelling under mechanical support from left ventricular assist devices.Front Cardiovasc Med. 2023 Aug 2;10:1212875. doi: 10.3389/fcvm.2023.1212875. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37600037 Free PMC article. Review.
-
Myocardial Recovery in the Systemic Context: A Philosophic Shift for the Heart Failure Subspecialty to Optimize Patient Care.Methodist Debakey Cardiovasc J. 2024 Aug 20;20(4):98-108. doi: 10.14797/mdcvj.1416. eCollection 2024. Methodist Debakey Cardiovasc J. 2024. PMID: 39184157 Free PMC article. Review.
-
Left ventricular functional improvement appears to contribute to lower rates of device thrombosis in patients on durable mechanical circulatory support.J Heart Lung Transplant. 2023 Jul;42(7):853-858. doi: 10.1016/j.healun.2023.03.004. Epub 2023 Mar 13. J Heart Lung Transplant. 2023. PMID: 37086251 Free PMC article.
-
Need for Unstructured Preimplantation Data to Predict Myocardial Recovery in Patients With a Left Ventricular Assist Device.J Am Heart Assoc. 2022 Mar;11(5):e025530. doi: 10.1161/JAHA.122.025530. Epub 2022 Feb 22. J Am Heart Assoc. 2022. PMID: 35191319 Free PMC article. No abstract available.
References
-
- Frazier OH. First use of an untethered, vented electric left ventricular assist device for long-term support. Circulation. 1994;89:2908–14. - PubMed
-
- Wever-Pinzon O, Drakos SG, McKellar SH, Horne BD, Caine WT, Kfoury AG, Li DY, Fang JC, Stehlik J and Selzman CH. Cardiac Recovery During Long-Term Left Ventricular Assist Device Support. J Am Coll Cardiol. 2016;68:1540–53. - PubMed
-
- Topkara VK, Garan AR, Fine B, Godier-Furnemont AF, Breskin A, Cagliostro B, Yuzefpolskaya M, Takeda K, Takayama H, Mancini DM, et al. Myocardial Recovery in Patients Receiving Contemporary Left Ventricular Assist Devices: Results From the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS). Circulation Heart failure. 2016;9. PMC4943678. - PMC - PubMed
-
- Maybaum S, Mancini D, Xydas S, Starling RC, Aaronson K, Pagani FD, Miller LW, Margulies K, McRee S, Frazier OH, et al. Cardiac improvement during mechanical circulatory support: a prospective multicenter study of the LVAD Working Group. Circulation. 2007;115:2497–505. - PubMed
-
- Birks EJ, Tansley PD, Hardy J, George RS, Bowles CT, Burke M, Banner NR, Khaghani A and Yacoub MH. Left ventricular assist device and drug therapy for the reversal of heart failure. N Engl J Med. 2006;355:1873–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
