

Clinical Features, Endoscopic Findings, and Predictive Factors for Mortality in Tissue-Invasive Gastrointestinal Cytomegalovirus Disease between Immunocompetent and Immunocompromised Patients
- PMID: 33897776
- PMCID: PMC8052155
- DOI: 10.1155/2021/8886525
Clinical Features, Endoscopic Findings, and Predictive Factors for Mortality in Tissue-Invasive Gastrointestinal Cytomegalovirus Disease between Immunocompetent and Immunocompromised Patients
Abstract
Background and aims: Tissue-invasive gastrointestinal cytomegalovirus (TI-GI CMV) disease is common in immunocompromised patients, but the increasing prevalence in immunocompetent patients has been reported. This study compared the clinical manifestations, endoscopic features, treatment outcomes, and predictors for inhospital mortality of TI-GI CMV between immunocompromised and immunocompetent patients.
Methods: Patients with HIV infection, malignancy, or receiving immunosuppressive agents (chemotherapy, high dose, or long-term corticosteroids) were defined as the immunocompromised group. Demographic and inhospital mortality data were obtained and retrospectively analyzed.
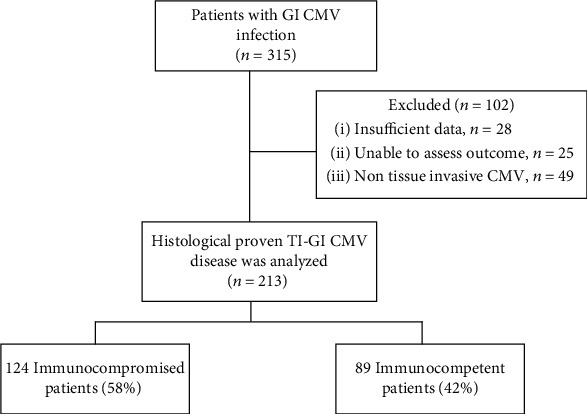
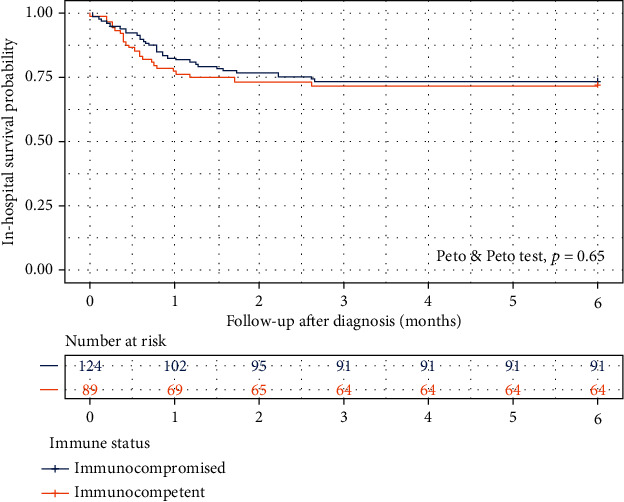
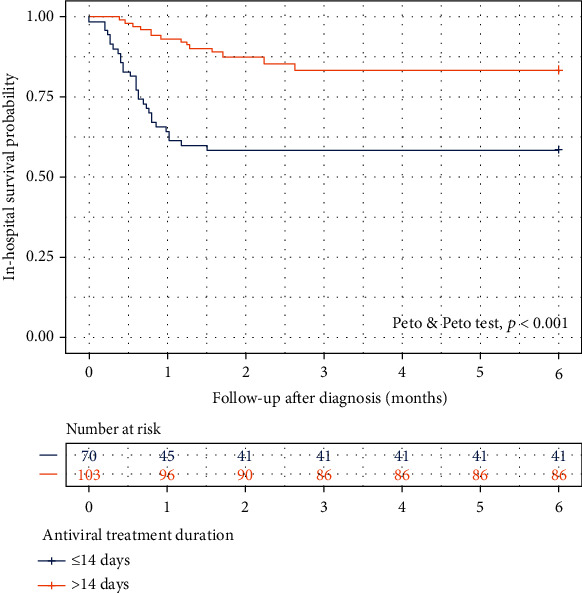
Results: A total of 213 patients (89 immunocompetent) with histologically confirmed TI-GI CMV were enrolled. Immunocompetent patients were older (70 vs. 52 years; p < 0.001), had more GI bleeding as a presenting symptom (47.2% vs. 29.0%; p = 0.010), and shorter symptom onset (2 vs. 14 days, p = 0.018). Concomitant extra-GI involvement was only seen in the immunocompromised group (6.5% vs. 0%; p = 0.02). Diffuse GI tract (14.5% vs. 4.5%; p = 0.032) and esophageal involvement (14.5% vs. 5.6%; p = 0.046) were more frequent in the immunocompromised, while small bowel involvement was more frequent in the immunocompetent group (19.1% vs. 8.1%; p = 0.029). An overall inhospital mortality was 27.7%. There was no significant difference in inhospital survival probability between the two groups (Peto-Peto test, p = 0.65). ICU admission (hazard ratio [HR] 7.21; 95% CI 2.55-20.36), sepsis or shock (HR 1.98; 95% CI 1.08-3.66), malnutrition (HR 2.62; 95% CI 1.05-7.01), and receiving chemotherapy (HR 5.2; 95% CI 1.89-14.29) were independent factors for inhospital mortality. Antiviral treatment for more than 14 days was the only protective factor to improve survival (Peto-Peto test, p < 0.001).
Conclusions: Immunocompetent and immunocompromised patients with TI-GI CMV disease had distinct clinical and endoscopic characteristics. There was no significant difference in the inhospital mortality between the two groups. The factors for mortality were ICU admission, sepsis/shock, malnutrition, and receiving chemotherapy. Early diagnosis and initiation of antiviral treatment might improve the survival probability.
Copyright © 2021 Panu Wetwittayakhlang et al.
Conflict of interest statement
All authors declare no conflict of interest related to the present study.
Figures
Similar articles
-
Comparative Analysis of Cytomegalovirus Gastrointestinal Disease in Immunocompetent and Immunocompromised Patients.Viruses. 2024 Mar 14;16(3):452. doi: 10.3390/v16030452. Viruses. 2024. PMID: 38543817 Free PMC article.
-
Patient characteristics, clinical manifestations, prognosis, and factors associated with gastrointestinal cytomegalovirus infection in immunocompetent patients.BMC Gastroenterol. 2020 Jan 30;20(1):22. doi: 10.1186/s12876-020-1174-y. BMC Gastroenterol. 2020. PMID: 32000707 Free PMC article.
-
Cytomegalovirus Diseases of the Gastrointestinal Tract.Viruses. 2022 Feb 8;14(2):352. doi: 10.3390/v14020352. Viruses. 2022. PMID: 35215942 Free PMC article.
-
Cytomegalovirus Diseases of the Gastrointestinal Tract in Immunocompetent Patients: A Narrative Review.Viruses. 2024 Feb 23;16(3):346. doi: 10.3390/v16030346. Viruses. 2024. PMID: 38543712 Free PMC article. Review.
-
Reactivated cytomegalovirus proctitis in an immunocompetent patient presenting as nosocomial diarrhea: a case report and literature review.BMC Infect Dis. 2017 Feb 1;17(1):113. doi: 10.1186/s12879-017-2218-y. BMC Infect Dis. 2017. PMID: 28143418 Free PMC article. Review.
Cited by
-
Cytomegalovirus Infection of the Gastrointestinal Tract in Patients on Hemodialysis: A Case Report and Literature Review.Cureus. 2024 Jul 9;16(7):e64129. doi: 10.7759/cureus.64129. eCollection 2024 Jul. Cureus. 2024. PMID: 39119410 Free PMC article.
-
Viral esophagitis in non-human immunodeficiency virus patients: a case-control study.Transl Gastroenterol Hepatol. 2024 Mar 29;9:19. doi: 10.21037/tgh-23-44. eCollection 2024. Transl Gastroenterol Hepatol. 2024. PMID: 38716211 Free PMC article.
-
Comparative Analysis of Cytomegalovirus Gastrointestinal Disease in Immunocompetent and Immunocompromised Patients.Viruses. 2024 Mar 14;16(3):452. doi: 10.3390/v16030452. Viruses. 2024. PMID: 38543817 Free PMC article.
-
Coexisting cytomegalovirus colitis in an immunocompetent patient with Clostridioides difficile colitis: A case report.World J Clin Cases. 2023 Apr 6;11(10):2343-2348. doi: 10.12998/wjcc.v11.i10.2343. World J Clin Cases. 2023. PMID: 37122504 Free PMC article.
-
Immunohistochemistry Staining-Proven Cytomegalovirus Colitis in Living Donor Liver Transplantation.Viruses. 2022 Dec 30;15(1):115. doi: 10.3390/v15010115. Viruses. 2022. PMID: 36680155 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
