

Understanding the impact of high-risk human papillomavirus on oropharyngeal squamous cell carcinomas in Taiwan: A retrospective cohort study
- PMID: 33891627
- PMCID: PMC8064583
- DOI: 10.1371/journal.pone.0250530
Understanding the impact of high-risk human papillomavirus on oropharyngeal squamous cell carcinomas in Taiwan: A retrospective cohort study
Abstract
Background and objectives: Human papillomavirus (HPV)-driven oropharyngeal squamous cell carcinoma (OPSCC) is increasing globally. In Taiwan, HPV-positive OPSCC is obscured by tobacco, alcohol, and betel quid use. We investigated the role of high-risk HPV (hrHPV) in a large retrospective Taiwan OPSCC cohort.
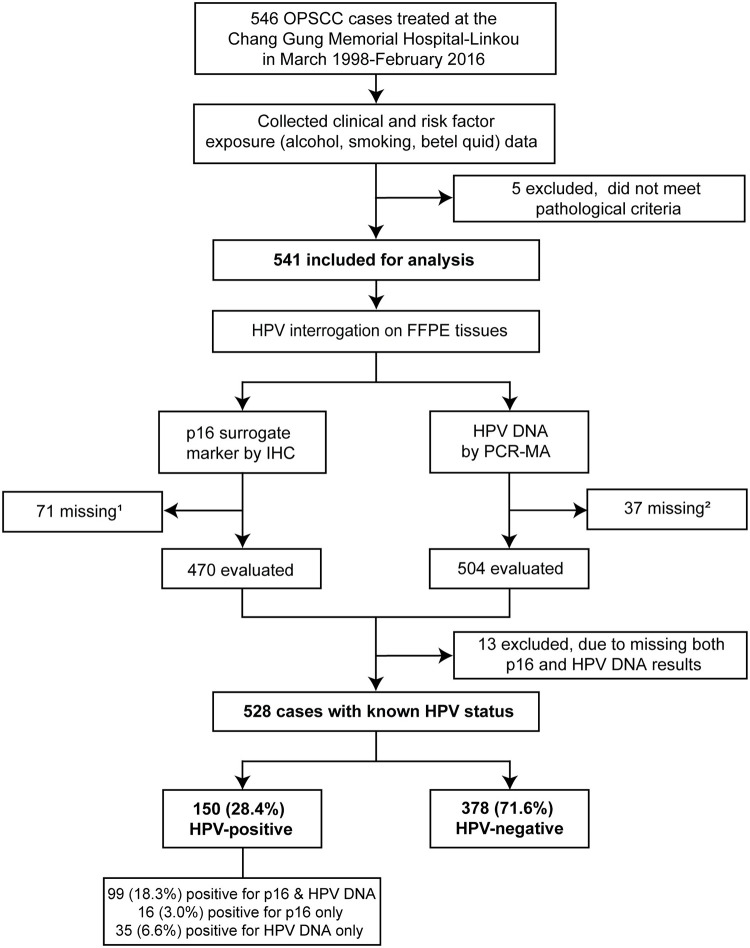
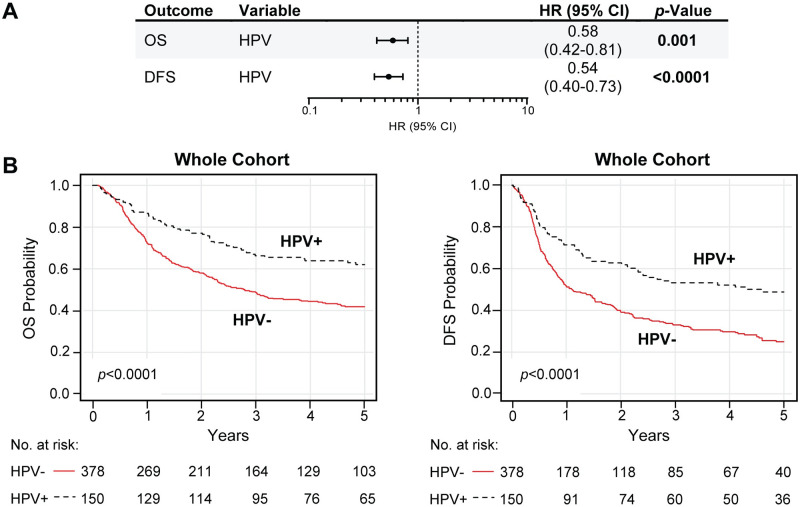
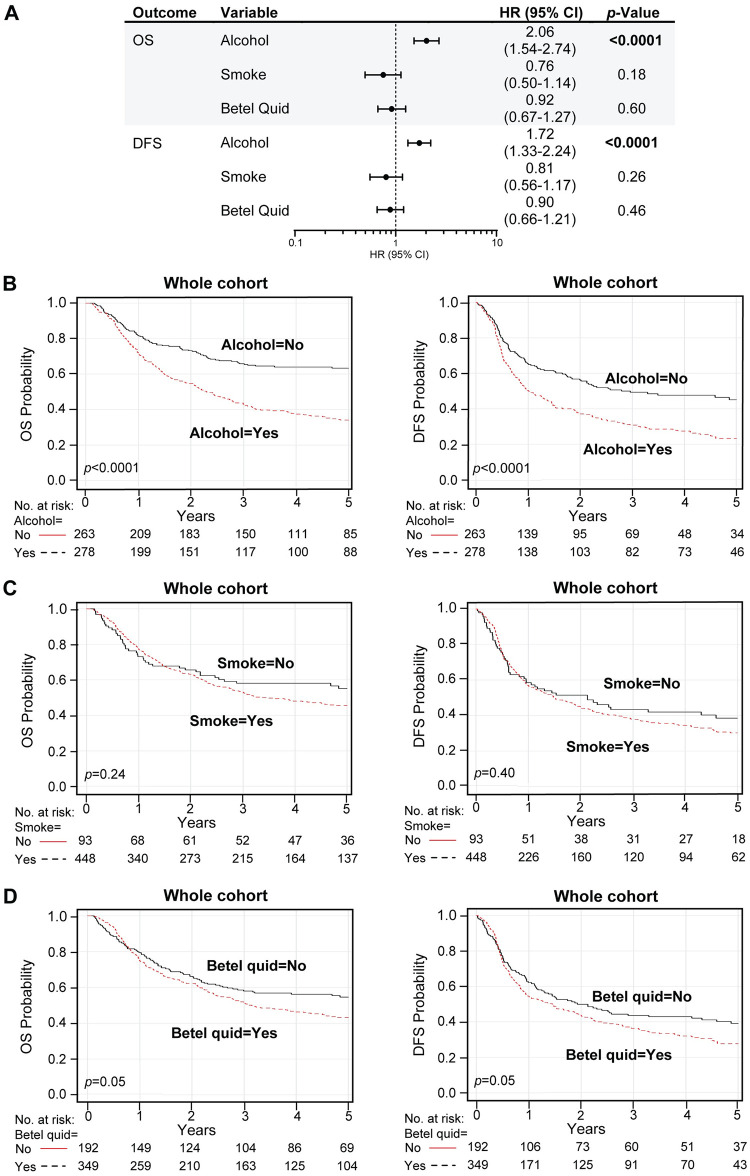
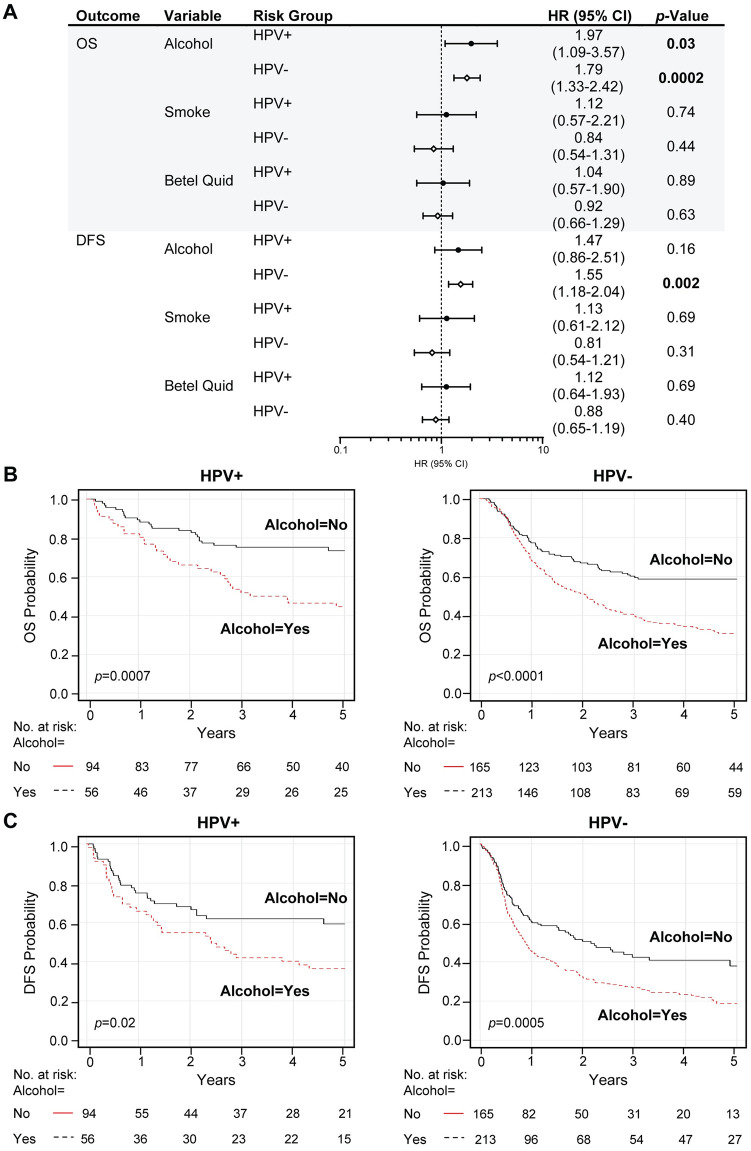
Methods and results: The cohort of 541 OPSCCs treated at Chang Gung Memorial Hospital from 1998-2016 consisted of 507 men (94%) and 34 women (6%). Most used tobacco (81%), alcohol (51%), and betel quid (65%). Formalin-fixed, paraffin-embedded tissue was used for p16 staining (a surrogate marker for HPV) and testing for HPV DNA presence and type by Multiplex HPV PCR-MassArray. HPV DNA and/or p16 staining (HPV-positive) was found in 28.4% (150/528) tumors. p16 and HPV DNA were strongly correlated (F < 0.0001). HPV16 was present in 82.8%, and HPV58 in 7.5% of HPV-positive tumors. HPV was associated with higher age (55.5 vs. 52.7 years, p = 0.004), lower T-stage (p = 0.008) better overall survival (OS) (hazard ratio [HR] 0.58 [95% CI 0.42-0.81], p = 0.001), and disease-free survival (DFS) (HR 0.54 [95% CI 0.40-0.73], p < 0.0001). Alcohol was strongly associated with recurrence and death (OS: HR 2.06 [95% CI 1.54-2.74], p < 0.0001; DFS: HR 1.72 [95% CI 1.33-2.24], p < 0.0001). OS and DFS in HPV-positive cases decreased for alcohol users (p < 0.0001). Obscured by the strong alcohol effect, predictive associations were not found for tobacco or betel quid.
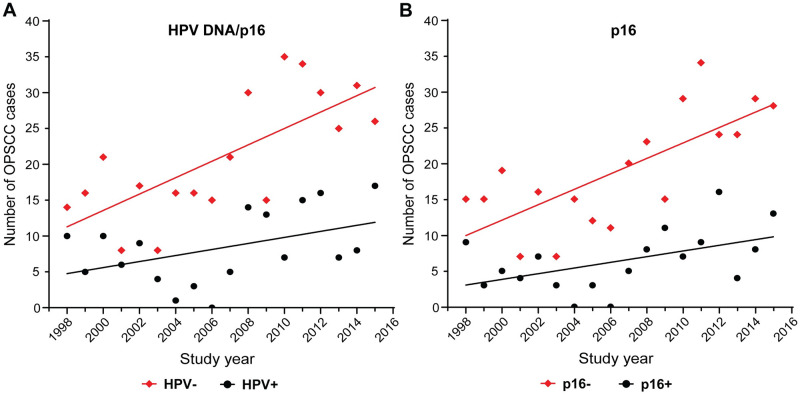
Conclusions: As with HPV-positive OPSCC globally, HPV is an increasingly important etiological factor in Taiwanese OPSCC. HPV-positive OPSCC has considerable survival benefit, but this is reduced by alcohol, tobacco, and betel quid use. hrHPV is a cancer risk factor in males and females. Vaccinating both sexes with a multivalent vaccine including HPV58, combined with alcohol and tobacco cessation policies will be effective cancer-prevention public health strategies in Taiwan.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Extracapsular extension of neck nodes and absence of human papillomavirus 16-DNA are predictors of impaired survival in p16-positive oropharyngeal squamous cell carcinoma.Cancer. 2020 Jan 1;126(9):1856-1872. doi: 10.1002/cncr.32667. Epub 2020 Feb 7. Cancer. 2020. PMID: 32032442
-
The prognostic role of sex, race, and human papillomavirus in oropharyngeal and nonoropharyngeal head and neck squamous cell cancer.Cancer. 2017 May 1;123(9):1566-1575. doi: 10.1002/cncr.30353. Epub 2017 Feb 27. Cancer. 2017. PMID: 28241096 Free PMC article.
-
The evolving landscape of human papillomavirus-related oropharyngeal squamous cell carcinoma at a single institution in Northern Italy.Acta Otorhinolaryngol Ital. 2019 Feb;39(1):9-17. doi: 10.14639/0392-100X-1905. Acta Otorhinolaryngol Ital. 2019. PMID: 30936574 Free PMC article.
-
Advances in Diagnosis and Multidisciplinary Management of Oropharyngeal Squamous Cell Carcinoma: State of the Art.Radiographics. 2019 Nov-Dec;39(7):2055-2068. doi: 10.1148/rg.2019190007. Epub 2019 Oct 11. Radiographics. 2019. PMID: 31603733 Review.
-
The relation between human papillomavirus (HPV) and oropharyngeal cancer: a review.PeerJ. 2023 Jun 26;11:e15568. doi: 10.7717/peerj.15568. eCollection 2023. PeerJ. 2023. PMID: 37397013 Free PMC article. Review.
Cited by
-
HPV-Related Oropharyngeal Cancer in Southern Thailand: Proportion Trend and Survival Outcome.Asian Pac J Cancer Prev. 2024 Jan 1;25(1):57-64. doi: 10.31557/APJCP.2024.25.1.57. Asian Pac J Cancer Prev. 2024. PMID: 38285767 Free PMC article.
-
Incremental net benefit of extending human papillomavirus vaccine to boys in oropharyngeal cancer burden: Meta-analysis of cost-effectiveness studies.J Dent Sci. 2024 Oct;19(4):2045-2056. doi: 10.1016/j.jds.2024.05.032. Epub 2024 Jun 8. J Dent Sci. 2024. PMID: 39347094 Free PMC article.
-
A predictive model for advanced oropharyngeal cancer patients treated with chemoradiation.BMC Cancer. 2022 Jun 5;22(1):615. doi: 10.1186/s12885-022-09732-9. BMC Cancer. 2022. PMID: 35659619 Free PMC article.
-
Application of Carotid Duplex Ultrasonography in the Surveillance of Carotid Artery Stenosis after Neck Irradiation.Rev Cardiovasc Med. 2022 Jun 27;23(7):240. doi: 10.31083/j.rcm2307240. eCollection 2022 Jul. Rev Cardiovasc Med. 2022. PMID: 39076899 Free PMC article. Review.
-
Update on the Epidemiological Features and Clinical Implications of Human Papillomavirus Infection (HPV) and Human Immunodeficiency Virus (HIV) Coinfection.Microorganisms. 2022 May 18;10(5):1047. doi: 10.3390/microorganisms10051047. Microorganisms. 2022. PMID: 35630489 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
