

Primary central nervous system Hodgkin's lymphoma: a case report
- PMID: 33874776
- PMCID: PMC8060762
- DOI: 10.1177/0300060521999533
Primary central nervous system Hodgkin's lymphoma: a case report
Abstract
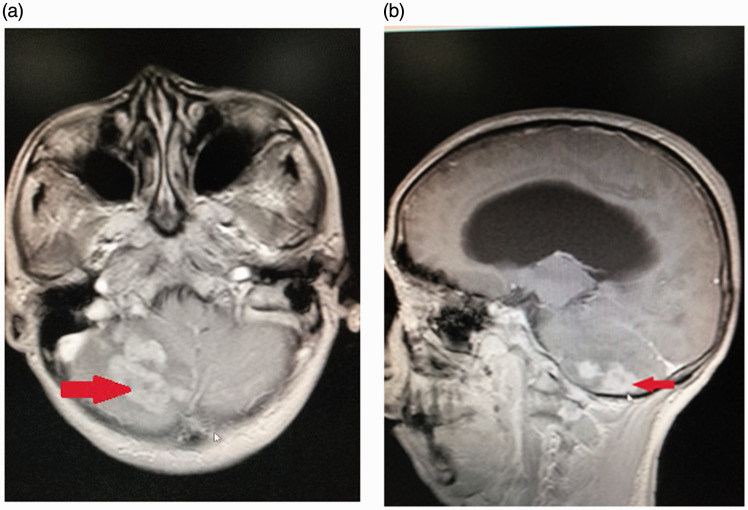
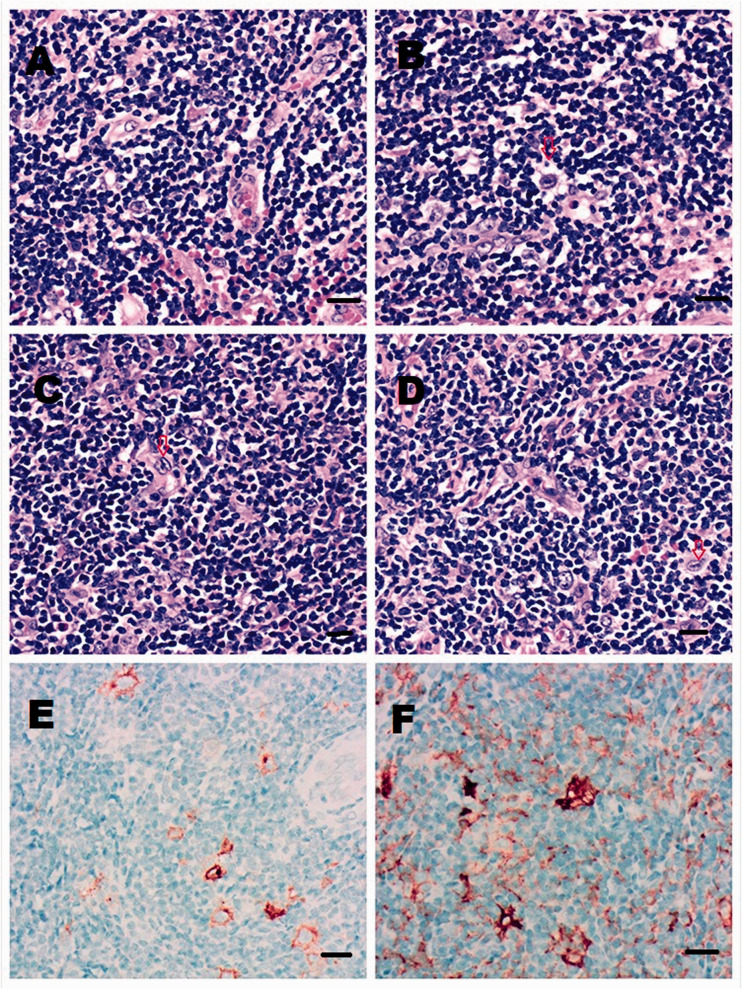
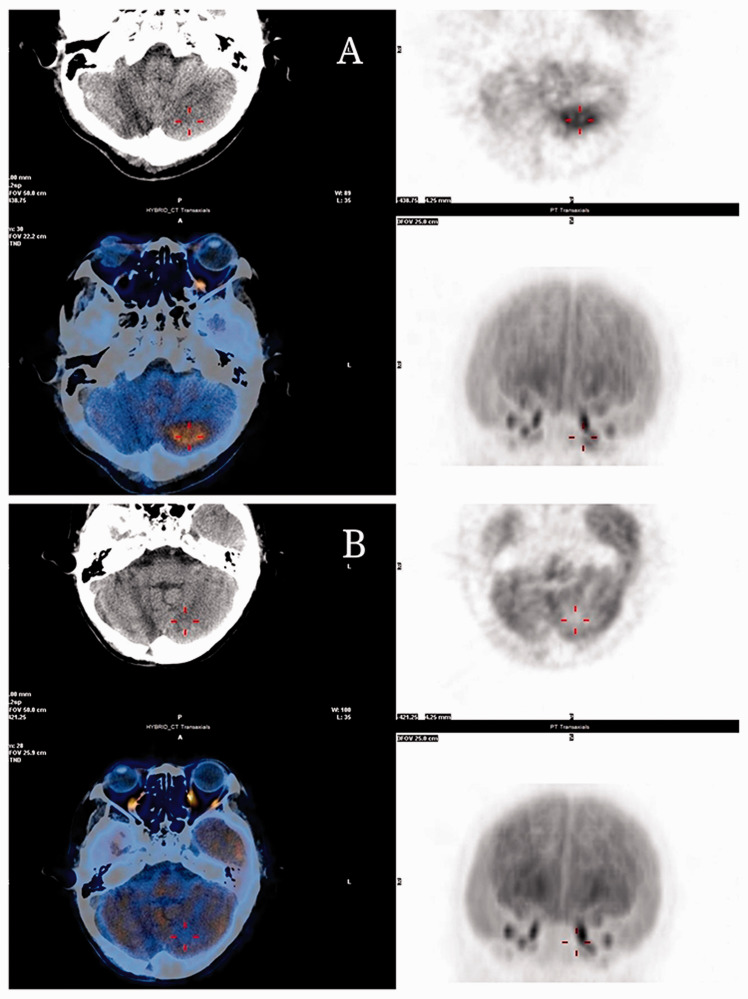
Primary central nervous system Hodgkin's lymphoma (CNS-HL) is extremely rare. This current case report describes a 60-year-old male patient that presented with numbness of the left lower extremity and worsening headache. After a full range of investigations and a partial resection of the right cerebellum, external ventricular drainage reservoir placement and cranioplasty, he was diagnosed with primary CNS-HL. The patient was treated with 3 g/m2 methotrexate (intravenous [i.v.], once a day, day 1) and 1 g/m2 cytarabine (i.v., every 12 h, days 2 + 3), followed by anti-programmed cell death protein 1 antibodies (200 mg sintilimab, i.v., once a day, day 1, every 3 weeks). After six courses of treatment with intrathecal injections of 50 mg cytarabine (once a day, day 1) and 5 mg dexamethasone (once a day, day 1), there was no residual lesion on cranial magnetic resonance imaging. No significant drug-related adverse events were observed. The patient has been followed up every 3 months and no relapse has occurred.
Keywords: Hodgkin's lymphoma; Primary central nervous system; prognosis; programmed cell death-1; treatment.
Conflict of interest statement
Figures
Similar articles
-
[Therapeutic management of central nervous system lymphomas in a single hematological institute].Orv Hetil. 2009 Oct 18;150(42):1937-44. doi: 10.1556/OH.2009.28703. Orv Hetil. 2009. PMID: 19812012 Hungarian.
-
High-dose cytarabine plus high-dose methotrexate versus high-dose methotrexate alone in patients with primary CNS lymphoma: a randomised phase 2 trial.Lancet. 2009 Oct 31;374(9700):1512-20. doi: 10.1016/S0140-6736(09)61416-1. Epub 2009 Sep 18. Lancet. 2009. PMID: 19767089 Clinical Trial.
-
Primary non-Hodgkin's lymphoma of the CNS treated with CHOD/BVAM or BVAM chemotherapy before radiotherapy: long-term survival and prognostic factors.Int J Radiat Oncol Biol Phys. 2004 Jun 1;59(2):501-8. doi: 10.1016/j.ijrobp.2003.11.001. Int J Radiat Oncol Biol Phys. 2004. PMID: 15145169
-
A Rare Case of Spontaneous Remission and Relapse of a Primary Central Nervous System Lymphoma.Acta Med Port. 2018 Dec 28;31(12):777-783. doi: 10.20344/amp.10198. Epub 2018 Dec 28. Acta Med Port. 2018. PMID: 30684376 Review.
-
Management of Hodgkin's lymphoma with midbrain involvement: A case report and review of literature.Hematology. 2015 Jun;20(5):272-5. doi: 10.1179/1607845414Y.0000000190. Epub 2014 Aug 18. Hematology. 2015. PMID: 25133862 Review.
Cited by
-
Posterior fossa Hodgkin's lymphoma radiographically mimicking an arteriovenous malformation: illustrative case.J Neurosurg Case Lessons. 2024 Jul 22;8(4):CASE24238. doi: 10.3171/CASE24238. Print 2024 Jul 22. J Neurosurg Case Lessons. 2024. PMID: 39038366 Free PMC article.
-
Intracranial Involvement of Systemic Hodgkin Lymphoma: A Case Report and Literature Review.Brain Tumor Res Treat. 2024 Jan;12(1):63-69. doi: 10.14791/btrt.2023.0041. Brain Tumor Res Treat. 2024. PMID: 38317490 Free PMC article.
-
Hodgkin Lymphoma Involving the Brain: Report of a Rare Case.Cureus. 2024 Jan 12;16(1):e52173. doi: 10.7759/cureus.52173. eCollection 2024 Jan. Cureus. 2024. PMID: 38344611 Free PMC article.
References
-
- Hwang CY, Song YJ, Kim DC, et al.. Primary cerebellar Hodgkin's lymphoma. J Korean Neurosurg Soc 2007; 42: 149–152.
-
- Cecyn KZ, Chaves EM, Oliveira JS. Primary central nervous system involvement in classical Hodgkin’s lymphoma: Case report and review of the literature. J Blood Lymph 2017; 8: 196. DOI: 10.4172/21657831.1000196.
-
- Szelemej PA, Bigder MG, Krcek J, et al. . Treatment and long-term follow-up of primary CNS classical Hodgkin's lymphoma – A case report and review of the literature. Interdiscip Neurosurg 2017; 9: 30–33. DOI: 10.1016/j.inat.2017.02.002
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
