

The Role of Oxidative Stress in Hyperuricemia and Xanthine Oxidoreductase (XOR) Inhibitors
- PMID: 33854690
- PMCID: PMC8019370
- DOI: 10.1155/2021/1470380
The Role of Oxidative Stress in Hyperuricemia and Xanthine Oxidoreductase (XOR) Inhibitors
Abstract
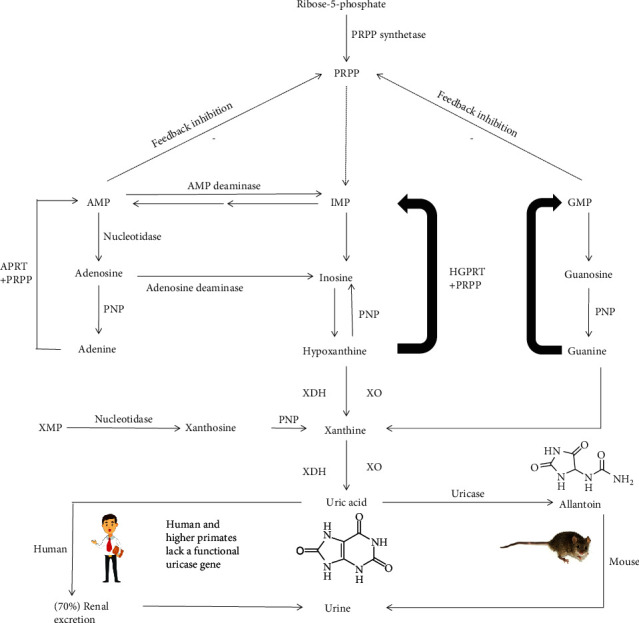
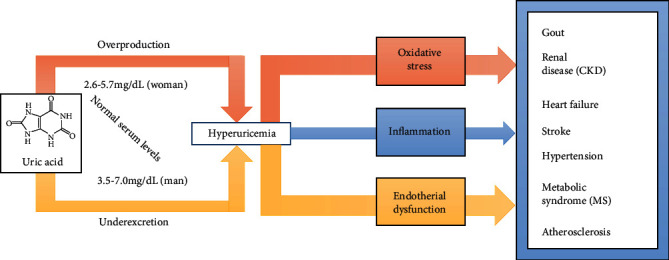
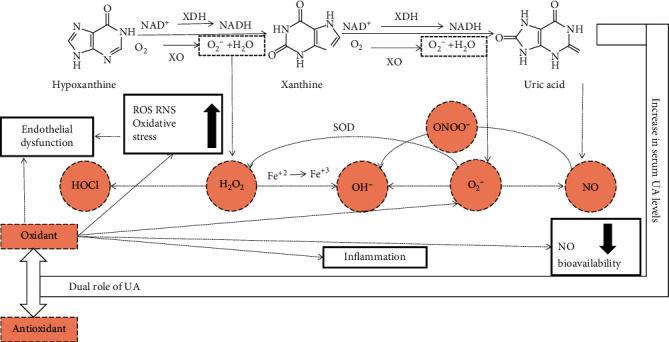
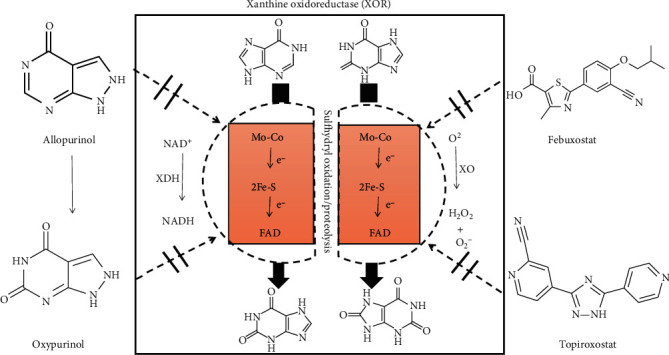
Uric acid is the end product of purine metabolism in humans. Hyperuricemia is a metabolic disease caused by the increased formation or reduced excretion of serum uric acid (SUA). Alterations in SUA homeostasis have been linked to a number of diseases, and hyperuricemia is the major etiologic factor of gout and has been correlated with metabolic syndrome, cardiovascular disease, diabetes, hypertension, and renal disease. Oxidative stress is usually defined as an imbalance between free radicals and antioxidants in our body and is considered to be one of the main causes of cell damage and the development of disease. Studies have demonstrated that hyperuricemia is closely related to the generation of reactive oxygen species (ROS). In the human body, xanthine oxidoreductase (XOR) catalyzes the oxidative hydroxylation of hypoxanthine to xanthine to uric acid, with the accompanying production of ROS. Therefore, XOR is considered a drug target for the treatment of hyperuricemia and gout. In this review, we discuss the mechanisms of uric acid transport and the development of hyperuricemia, emphasizing the role of oxidative stress in the occurrence and development of hyperuricemia. We also summarize recent advances and new discoveries in XOR inhibitors.
Copyright © 2021 Ning Liu et al.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Hyperuricemia-Related Diseases and Xanthine Oxidoreductase (XOR) Inhibitors: An Overview.Med Sci Monit. 2016 Jul 17;22:2501-12. doi: 10.12659/msm.899852. Med Sci Monit. 2016. PMID: 27423335 Free PMC article. Review.
-
New insights into purine metabolism in metabolic diseases: role of xanthine oxidoreductase activity.Am J Physiol Endocrinol Metab. 2020 Nov 1;319(5):E827-E834. doi: 10.1152/ajpendo.00378.2020. Epub 2020 Sep 7. Am J Physiol Endocrinol Metab. 2020. PMID: 32893671 Review.
-
The double faced role of xanthine oxidoreductase in cancer.Acta Pharmacol Sin. 2022 Jul;43(7):1623-1632. doi: 10.1038/s41401-021-00800-7. Epub 2021 Nov 22. Acta Pharmacol Sin. 2022. PMID: 34811515 Free PMC article. Review.
-
The role of xanthine oxidoreductase and uric acid in metabolic syndrome.Biochim Biophys Acta Mol Basis Dis. 2018 Aug;1864(8):2557-2565. doi: 10.1016/j.bbadis.2018.05.003. Epub 2018 May 5. Biochim Biophys Acta Mol Basis Dis. 2018. PMID: 29733945 Review.
-
Mechanistic insights into xanthine oxidoreductase from development studies of candidate drugs to treat hyperuricemia and gout.J Biol Inorg Chem. 2015 Mar;20(2):195-207. doi: 10.1007/s00775-014-1210-x. Epub 2014 Dec 12. J Biol Inorg Chem. 2015. PMID: 25501928 Free PMC article. Review.
Cited by
-
Ethanolic Extract from Limonia acidissima L. Fruit Attenuates Serum Uric Acid Level via URAT1 in Potassium Oxonate-Induced Hyperuricemic Rats.Pharmaceuticals (Basel). 2023 Mar 9;16(3):419. doi: 10.3390/ph16030419. Pharmaceuticals (Basel). 2023. PMID: 36986518 Free PMC article.
-
Renal interstitial fibrotic assessment using non-Gaussian diffusion kurtosis imaging in a rat model of hyperuricemia.BMC Med Imaging. 2024 Apr 3;24(1):78. doi: 10.1186/s12880-024-01259-8. BMC Med Imaging. 2024. PMID: 38570748 Free PMC article.
-
Oxidative Stress Underpins Clinical, Social, and Genetic Risk Factors for Atherosclerotic Cardiovascular Disease.Clin Med Insights Cardiol. 2023 Apr 29;17:11795468231170779. doi: 10.1177/11795468231170779. eCollection 2023. Clin Med Insights Cardiol. 2023. PMID: 37153696 Free PMC article.
-
Extracellular vesicles isolated from hyperuricemia patients might aggravate airway inflammation of COPD via senescence-associated pathway.J Inflamm (Lond). 2022 Nov 2;19(1):18. doi: 10.1186/s12950-022-00315-w. J Inflamm (Lond). 2022. PMID: 36324164 Free PMC article.
-
Potential use of antioxidants for the treatment of chronic inflammatory diseases.Front Pharmacol. 2024 May 16;15:1378335. doi: 10.3389/fphar.2024.1378335. eCollection 2024. Front Pharmacol. 2024. PMID: 38818374 Free PMC article. Review.
References
-
- Scheele C. Examen chemicum calculi urinarii. Opuscula. 1776;2(73)
-
- Horbaczewski J. Synthese der Harnsäure. Monatshefte für Chemie. 1882;3(1):796–797.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
