

FDG-PET/CT in intensive care patients with bloodstream infection
- PMID: 33827655
- PMCID: PMC8028784
- DOI: 10.1186/s13054-021-03557-x
FDG-PET/CT in intensive care patients with bloodstream infection
Abstract
Background: 2-Deoxy-2-[18F]fluoro-D-glucose (FDG) positron emission tomography (PET)/computed tomography (CT) is an advanced imaging technique that can be used to examine the whole body for an infection focus in a single examination in patients with bloodstream infection (BSI) of unknown origin. However, literature on the use of this technique in intensive care patients is scarce. The purpose of this study was to evaluate the diagnostic yield of FDG-PET/CT in intensive care patients with BSI.
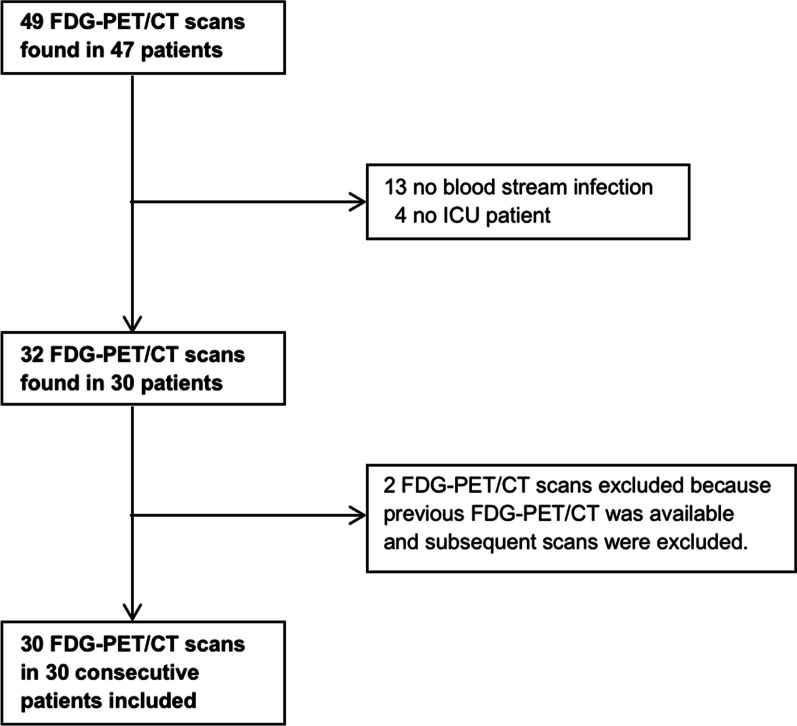
Methods: In this retrospective cohort study, all intensive care patients from our Dutch university medical center who had culture-proven BSI between 2010 and 2020 and underwent FDG-PET/CT to find the focus of infection were included. Diagnostic performance was calculated and logistic regression analysis was performed to evaluate the association between FDG-PET/CT outcome and C-reactive protein level (CRP), leukocyte count, duration of antibiotic treatment, duration of ICU stay, quality of FDG-PET/CT, and dependency on mechanical ventilation. In addition, the impact of FDG-PET/CT on clinical treatment was evaluated.
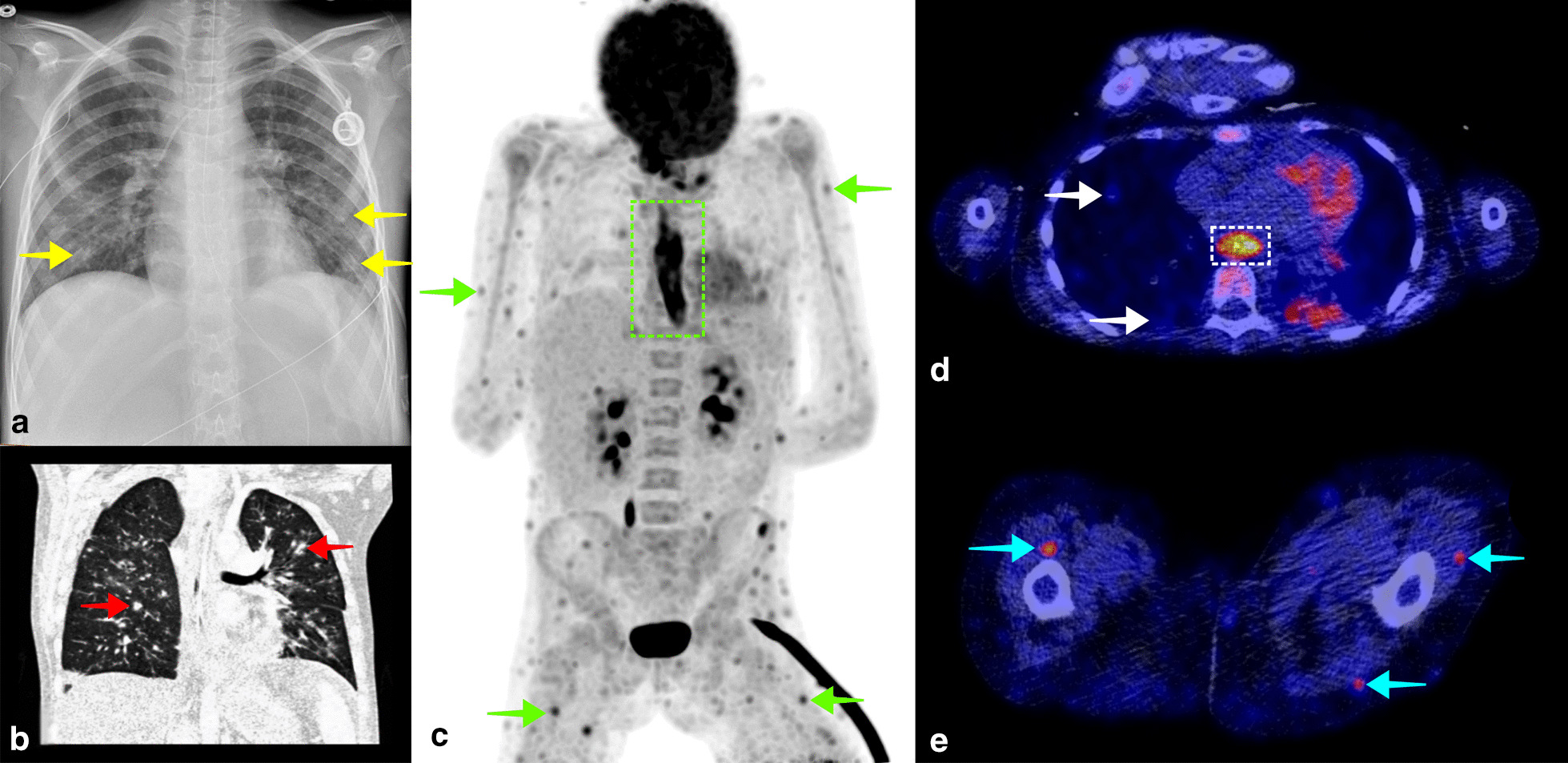
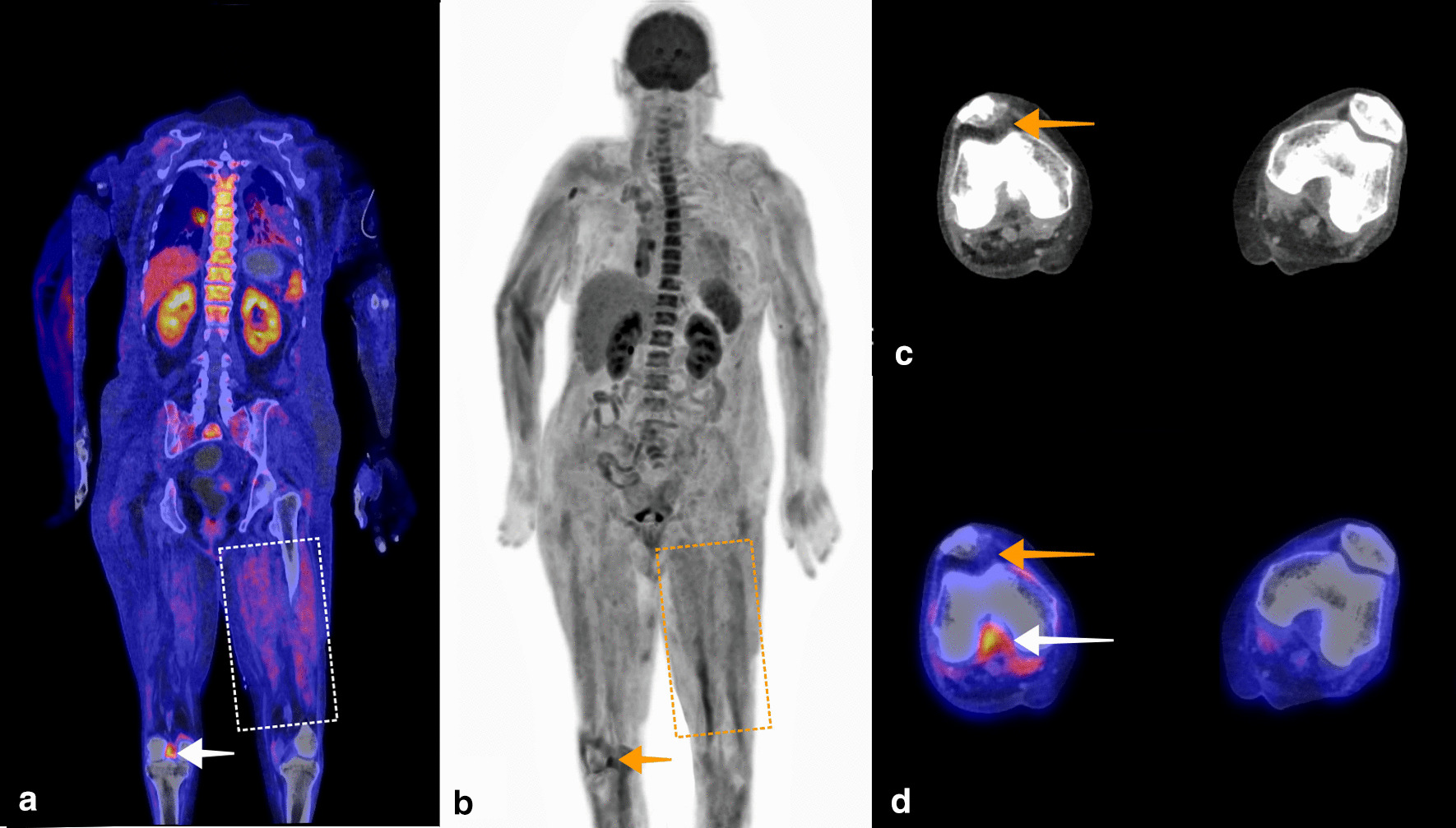
Results: 30 intensive care patients with BSI were included. In 21 patients, an infection focus was found on FDG-PET/CT which led to changes in clinical management in 14 patients. FDG-PET/CT achieved a sensitivity of 90.9% and specificity of 87.5% for identifying the focus of infection. Poor quality of the FDG-PET images significantly decreased the likelihood of finding an infection focus as compared to reasonable or good image quality (OR 0.16, P = 0.034). No other variables were significantly associated with FDG-PET/CT outcome. No adverse events during the FDG-PET/CT procedure were reported.
Conclusion: FDG-PET/CT has a high diagnostic yield for detecting the infection focus in patients with BSI admitted to intensive care. Poor PET image quality was significantly associated with a decreased likelihood of finding the infection focus in patients with BSI. This could be improved by adequate dietary preparation and cessation of intravenous glucose and glucose-regulating drugs. Recent advances in PET/CT technology enable higher image quality with shorter imaging time and may contribute to routinely performing FDG-PET/CT in intensive care patients with BSI of unknown origin.
Keywords: Bacteremia; Bloodstream infection; Candidemia; Fungemia; PET/CT; Sepsis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
FDG-PET/CT for Detecting an Infection Focus in Patients With Bloodstream Infection: Factors Affecting Diagnostic Yield.Clin Nucl Med. 2019 Feb;44(2):99-106. doi: 10.1097/RLU.0000000000002381. Clin Nucl Med. 2019. PMID: 30516689
-
Clinical implications of increased uptake in bone marrow and spleen on FDG-PET in patients with bacteremia.Eur J Nucl Med Mol Imaging. 2021 May;48(5):1467-1477. doi: 10.1007/s00259-020-05071-8. Epub 2020 Oct 26. Eur J Nucl Med Mol Imaging. 2021. PMID: 33106925 Free PMC article.
-
18F-FES PET/CT Influences the Staging and Management of Patients with Newly Diagnosed Estrogen Receptor-Positive Breast Cancer: A Retrospective Comparative Study with 18F-FDG PET/CT.Oncologist. 2019 Dec;24(12):e1277-e1285. doi: 10.1634/theoncologist.2019-0096. Epub 2019 Jul 23. Oncologist. 2019. PMID: 31337657 Free PMC article.
-
Evidence of Clinical Impact Supports a New Petition for Medicare Coverage of 2-[18F]Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography/Computed Tomography in the Evaluation of Staphylococcus aureus Bacteremia: A Focused Literature Review and Call to Action.Clin Infect Dis. 2022 Oct 12;75(8):1457-1461. doi: 10.1093/cid/ciac363. Clin Infect Dis. 2022. PMID: 35535794 Review.
-
Practice of 18F-FDG-PET/CT in ICU Patients: A Systematic Review.Semin Nucl Med. 2023 Nov;53(6):809-819. doi: 10.1053/j.semnuclmed.2023.05.003. Epub 2023 May 29. Semin Nucl Med. 2023. PMID: 37258380 Review.
Cited by
-
State of the art of 18F-FDG PET/CT application in inflammation and infection: a guide for image acquisition and interpretation.Clin Transl Imaging. 2021;9(4):299-339. doi: 10.1007/s40336-021-00445-w. Epub 2021 Jul 10. Clin Transl Imaging. 2021. PMID: 34277510 Free PMC article. Review.
-
[18F]FDG-PET/CT in mechanically ventilated critically ill patients with COVID-19 ARDS and persistent inflammation.Clin Transl Imaging. 2023;11(3):297-306. doi: 10.1007/s40336-023-00550-y. Epub 2023 Mar 12. Clin Transl Imaging. 2023. PMID: 37275950 Free PMC article.
-
[18F]FDG-PET/CT in patients with bacteremia: Clinical impact on patient management and outcome.Front Med (Lausanne). 2023 Mar 29;10:1157692. doi: 10.3389/fmed.2023.1157692. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37064040 Free PMC article. Review.
-
Positron Emission Tomography with Computed Tomography in Evaluations of Classical Fever of Unknown Origin and Length of Hospitalization: A 10-Year Medical Record Review of a Tertiary Hospital.Infect Chemother. 2023 Mar;55(1):22-28. doi: 10.3947/ic.2022.0082. Epub 2022 Oct 12. Infect Chemother. 2023. PMID: 36372950 Free PMC article.
-
Bacterial co-infection in COVID-19: a call to stay vigilant.PeerJ. 2024 Sep 19;12:e18041. doi: 10.7717/peerj.18041. eCollection 2024. PeerJ. 2024. PMID: 39308818 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
