

Fluorescence-Guided High-Grade Glioma Surgery More Than Four Hours After 5-Aminolevulinic Acid Administration
- PMID: 33767664
- PMCID: PMC7985355
- DOI: 10.3389/fneur.2021.644804
Fluorescence-Guided High-Grade Glioma Surgery More Than Four Hours After 5-Aminolevulinic Acid Administration
Abstract
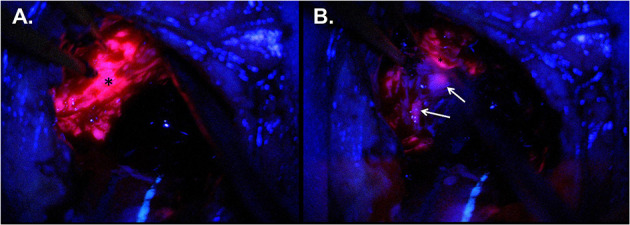
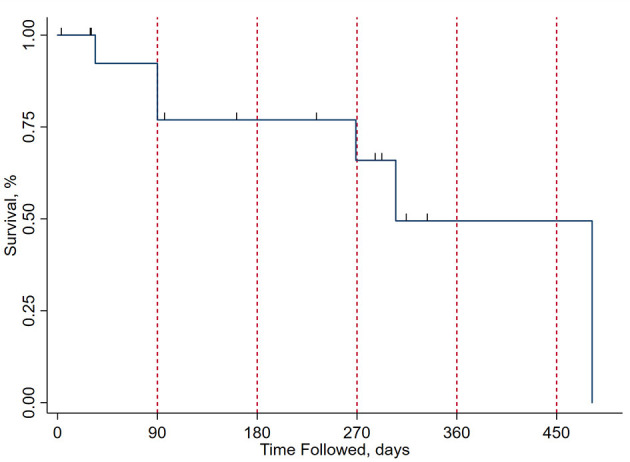
Background: Fluorescence-guided surgery (FGS) using 5-aminolevulic acid (5-ALA) is a widely used strategy for delineating tumor tissue from surrounding brain intraoperatively during high-grade glioma (HGG) resection. 5-ALA reaches peak plasma levels ~4 h after oral administration and is currently approved by the FDA for use 2-4 h prior to induction to anesthesia. Objective: To demonstrate that there is adequate intraoperative fluorescence in cases undergoing surgery more than 4 h after 5-ALA administration and compare survival and radiological recurrence to previous data. Methods: Retrospective analysis of HGG patients undergoing FGS more than 4 h after 5-ALA administration was performed at two institutions. Clinical, operative, and radiographic pre- and post-operative characteristics are presented. Results: Sixteen patients were identified, 6 of them female (37.5%), with mean (SD) age of 59.3 ± 11.5 years. Preoperative mean modified Rankin score (mRS) was 2 ± 1. All patients were dosed with 20 mg/kg 5-ALA the morning of surgery. Mean time to anesthesia induction was 425 ± 334 min. All cases had adequate intraoperative fluorescence. Eloquent cortex was involved in 12 cases (75%), and 13 cases (81.3%) had residual contrast enhancement on postoperative MRI. Mean progression-free survival was 5 ± 3 months. In the study period, 6 patients died (37.5%), mean mRS was 2.3 ± 1.3, Karnofsky score 71.9 ± 22.1, and NIHSS 3.9 ± 2.4. Conclusion: Here we demonstrate that 5-ALA-guided HGG resection can be performed safely more than 4 h after administration, with clinical results largely similar to previous reports. Relaxation of timing restrictions could improve procedure workflow in busy neurosurgical centers, without additional risk to patients.
Keywords: 5-ALA; brain tumors; fluorescence; glioblastomas; glioma; intraoperative imaging; neuro-oncology.
Copyright © 2021 Maragkos, Schüpper, Lakomkin, Sideras, Price, Baron, Hamilton, Haider, Lee, Hadjipanayis and Robin.
Conflict of interest statement
CH is a consultant for NX Development Corporation (NXDC) and Synaptive Medical. NXDC, a privately held company, markets Gleolan (5-ALA, aminolevulinic acid hydrochloride). Gleolan is an optical imaging agent approved for the visualization of malignant tissue during glioma surgery. CH is a consultant for NXDC and receives royalty payments for the sale of Gleolan. CH receives financial compensation as a consultant and lecturer for Synaptive (manufacturer of the 3D Synaptive MODUS V device). He has also received speaker fees by Carl Zeiss and Leica. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
5-Aminolevulinic acid for enhanced surgical visualization of high-grade gliomas: a prospective, multicenter study.J Neurosurg. 2021 Oct 8;136(6):1525-1534. doi: 10.3171/2021.5.JNS21310. Print 2022 Jun 1. J Neurosurg. 2021. PMID: 34624862
-
5-Aminolevulinic Acid-Shedding Light on Where to Focus.World Neurosurg. 2021 Jun;150:9-16. doi: 10.1016/j.wneu.2021.02.118. Epub 2021 Mar 5. World Neurosurg. 2021. PMID: 33684574 Review.
-
Optimization of high-grade glioma resection using 5-ALA fluorescence-guided surgery: A literature review and practical recommendations from the neuro-oncology club of the French society of neurosurgery.Neurochirurgie. 2019 Aug;65(4):164-177. doi: 10.1016/j.neuchi.2019.04.005. Epub 2019 May 21. Neurochirurgie. 2019. PMID: 31125558 Review.
-
Impact of the combination of 5-aminolevulinic acid-induced fluorescence with intraoperative magnetic resonance imaging-guided surgery for glioma.World Neurosurg. 2011 Jul-Aug;76(1-2):120-7. doi: 10.1016/j.wneu.2011.02.005. World Neurosurg. 2011. PMID: 21839963
-
5-Aminolevulinic acid-enhanced fluorescence-guided treatment of high-grade glioma using angled endoscopic blue light visualization: technical case series with preliminary follow-up.J Neurosurg. 2022 Mar 18;137(5):1378-1386. doi: 10.3171/2022.1.JNS212562. Print 2022 Nov 1. J Neurosurg. 2022. PMID: 35303704
Cited by
-
Updates in intraoperative strategies for enhancing intra-axial brain tumor control.Neuro Oncol. 2022 Nov 2;24(Suppl 6):S33-S41. doi: 10.1093/neuonc/noac170. Neuro Oncol. 2022. PMID: 36322098 Free PMC article. Review.
-
Iron Oxide Incorporated Conjugated Polymer Nanoparticles for Simultaneous Use in Magnetic Resonance and Fluorescent Imaging of Brain Tumors.Pharmaceutics. 2021 Aug 14;13(8):1258. doi: 10.3390/pharmaceutics13081258. Pharmaceutics. 2021. PMID: 34452219 Free PMC article.
-
Mechanisms of Resistance and Current Treatment Options for Glioblastoma Multiforme (GBM).Cancers (Basel). 2023 Apr 1;15(7):2116. doi: 10.3390/cancers15072116. Cancers (Basel). 2023. PMID: 37046777 Free PMC article. Review.
-
Clinically useful tumor fluorescence greater than 24 hours after 5-aminolevulinic acid administration.Surg Neurol Int. 2022 Mar 25;13:99. doi: 10.25259/SNI_836_2021. eCollection 2022. Surg Neurol Int. 2022. PMID: 35399905 Free PMC article.
-
Combined use of 5-ALA-induced protoporphyrin IX and chlorin e6 for fluorescence diagnostics and photodynamic therapy of skin tumors.Lasers Med Sci. 2024 Oct 31;39(1):266. doi: 10.1007/s10103-024-04219-4. Lasers Med Sci. 2024. PMID: 39477891
References
-
- van den Bent MJ, Brandes AA, Taphoorn MJ, Kros JM, Kouwenhoven MCM, Delattre JY, et al. . Adjuvant procarbazine, lomustine, and vincristine chemotherapy in newly diagnosed anaplastic oligodendroglioma: long-term follow-up of EORTC brain tumor group study 26951. J Clin Oncol. (2013) 31:344–350. 10.1200/JCO.2012.43.2229 - DOI - PubMed
-
- Chang S, Zhang P, Cairncross JG, Gilbert MR, Bahary JP, Dolinskas CA, et al. . Phase III randomized study of radiation and temozolomide versus radiation and nitrosourea therapy for anaplastic astrocytoma: results of NRG Oncology RTOG 9813. Neuro Oncol. (2017) 19:252–58. 10.1093/neuonc/now313 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources