

SARS-CoV-2 vaccination modelling for safe surgery to save lives: data from an international prospective cohort study
- PMID: 33761533
- PMCID: PMC7995808
- DOI: 10.1093/bjs/znab101
SARS-CoV-2 vaccination modelling for safe surgery to save lives: data from an international prospective cohort study
Abstract
Background: Preoperative SARS-CoV-2 vaccination could support safer elective surgery. Vaccine numbers are limited so this study aimed to inform their prioritization by modelling.
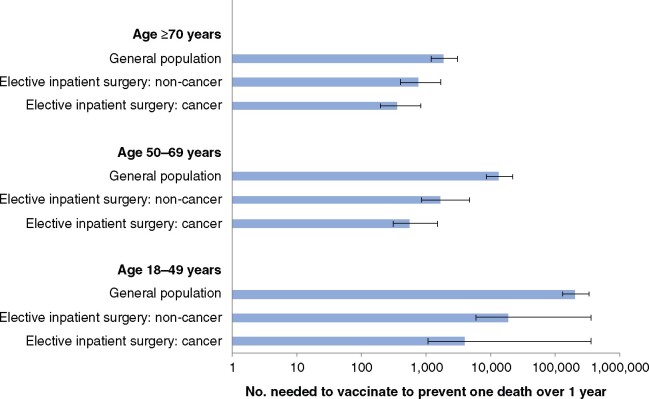
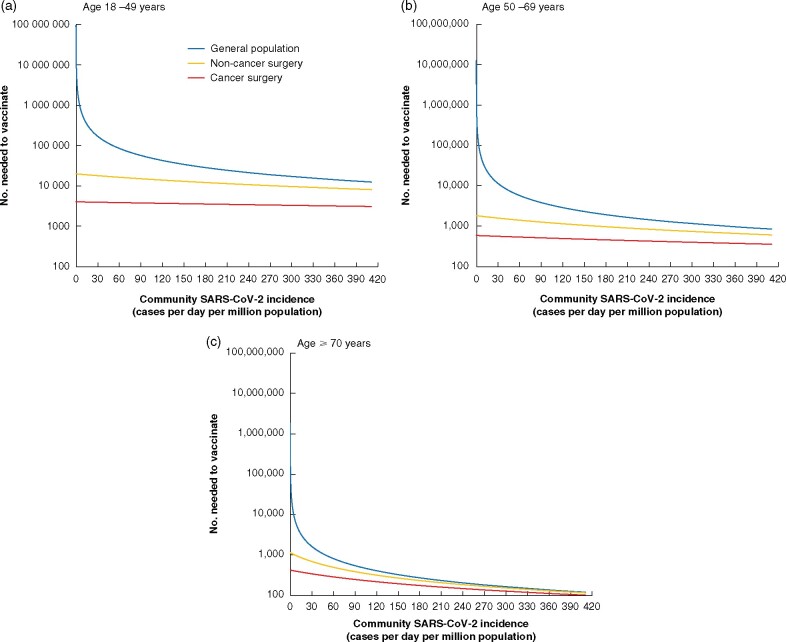
Methods: The primary outcome was the number needed to vaccinate (NNV) to prevent one COVID-19-related death in 1 year. NNVs were based on postoperative SARS-CoV-2 rates and mortality in an international cohort study (surgical patients), and community SARS-CoV-2 incidence and case fatality data (general population). NNV estimates were stratified by age (18-49, 50-69, 70 or more years) and type of surgery. Best- and worst-case scenarios were used to describe uncertainty.
Results: NNVs were more favourable in surgical patients than the general population. The most favourable NNVs were in patients aged 70 years or more needing cancer surgery (351; best case 196, worst case 816) or non-cancer surgery (733; best case 407, worst case 1664). Both exceeded the NNV in the general population (1840; best case 1196, worst case 3066). NNVs for surgical patients remained favourable at a range of SARS-CoV-2 incidence rates in sensitivity analysis modelling. Globally, prioritizing preoperative vaccination of patients needing elective surgery ahead of the general population could prevent an additional 58 687 (best case 115 007, worst case 20 177) COVID-19-related deaths in 1 year.
Conclusion: As global roll out of SARS-CoV-2 vaccination proceeds, patients needing elective surgery should be prioritized ahead of the general population.
Trial registration: ClinicalTrials.gov NCT04509986.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Elective Cancer Surgery in COVID-19-Free Surgical Pathways During the SARS-CoV-2 Pandemic: An International, Multicenter, Comparative Cohort Study.J Clin Oncol. 2021 Jan 1;39(1):66-78. doi: 10.1200/JCO.20.01933. Epub 2020 Oct 6. J Clin Oncol. 2021. PMID: 33021869 Free PMC article.
-
Effect of Pfizer/BioNTech and Oxford/AstraZeneca vaccines against COVID-19 morbidity and mortality in real-world settings at countrywide vaccination campaign in Saudi Arabia.Eur Rev Med Pharmacol Sci. 2021 Nov;25(22):7185-7191. doi: 10.26355/eurrev_202111_27271. Eur Rev Med Pharmacol Sci. 2021. PMID: 34859883
-
Prioritising COVID-19 vaccination in changing social and epidemiological landscapes: a mathematical modelling study.Lancet Infect Dis. 2021 Aug;21(8):1097-1106. doi: 10.1016/S1473-3099(21)00057-8. Epub 2021 Mar 31. Lancet Infect Dis. 2021. PMID: 33811817 Free PMC article.
-
The theoretical mortality risk of an asymptomatic patient with a negative SARS-CoV-2 test developing COVID-19 following elective orthopaedic surgery.Bone Joint J. 2020 Sep;102-B(9):1256-1260. doi: 10.1302/0301-620X.102B9.BJJ-2020-1147.R1. Epub 2020 Jul 6. Bone Joint J. 2020. PMID: 32627569 Review.
-
Targets and strategies for vaccine development against SARS-CoV-2.Biomed Pharmacother. 2021 May;137:111254. doi: 10.1016/j.biopha.2021.111254. Epub 2021 Jan 28. Biomed Pharmacother. 2021. PMID: 33550049 Free PMC article. Review.
Cited by
-
Estimated effect of COVID-19 vaccine in people with epilepsy.Epilepsy Behav. 2021 Aug;121(Pt A):108072. doi: 10.1016/j.yebeh.2021.108072. Epub 2021 May 19. Epilepsy Behav. 2021. PMID: 34058493 Free PMC article. No abstract available.
-
Risk of Early Postoperative Cardiovascular and Cerebrovascular Complication in Patients with Preoperative COVID-19 Undergoing Cancer Surgery.J Am Coll Surg. 2024 Jun 1;238(6):1085-1097. doi: 10.1097/XCS.0000000000001039. Epub 2024 Feb 13. J Am Coll Surg. 2024. PMID: 38348959
-
Evaluating Possible Mechanisms Linking Obesity to COVID-19: a Narrative Review.Obes Surg. 2022 May;32(5):1689-1700. doi: 10.1007/s11695-022-05933-0. Epub 2022 Feb 3. Obes Surg. 2022. PMID: 35113309 Free PMC article. Review.
-
Severity of Prior Coronavirus Disease 2019 is Associated With Postoperative Outcomes After Major Inpatient Surgery.Ann Surg. 2023 Nov 1;278(5):e949-e956. doi: 10.1097/SLA.0000000000006035. Epub 2023 Jul 21. Ann Surg. 2023. PMID: 37476995 Free PMC article.
-
The Impact of COVID-19 on Surgical Training: the Past, the Present and the Future.Indian J Surg. 2022 Apr;84(Suppl 1):131-138. doi: 10.1007/s12262-021-02964-2. Epub 2021 Jun 12. Indian J Surg. 2022. PMID: 34149230 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- Association of Upper Gastrointestinal Surgeons, British Association of Surgical Oncology, British Gynaecological Cancer Society, European Society of Coloproctology
- D43 TW010543/TW/FIC NIH HHS/United States
- NIHR Academy, Sarcoma UK
- CH/17/1/32804/BHF_/British Heart Foundation/United Kingdom
- 16.136.79/National Institute for Health Research (NIHR) Global Health Research Unit grant (NIHR
- F32 DK126232/DK/NIDDK NIH HHS/United States
- UK government to support global health research, Association of Coloproctology of Great Britain and Ireland, Bowel & Cancer Research, Bowel Disease Research Foundation
- 2018RIF_06/PANCREATICCANUK_/Pancreatic Cancer UK/United Kingdom
- 211122/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- The Urology Foundation, Vascular Society for Great Britain and Ireland, and Yorkshire Cancer Research
- PG/15/33/31394/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
- Diposit Digital de la Universitat de Barcelona - Access Free Full Text
- Europe PubMed Central
- ORBi (University of Liege)
- Ovid Technologies, Inc.
- PubMed Central
- Silverchair Information Systems
- University of Turin Instituional Repository AperTO - Free full text
- White Rose Research Online
- eScholarship, California Digital Library, University of California
Other Literature Sources
Medical
Research Materials
Miscellaneous
