

Early renal function trajectories, cytomegalovirus serostatus and long-term graft outcomes in kidney transplant recipients
- PMID: 33743617
- PMCID: PMC7981965
- DOI: 10.1186/s12882-021-02285-2
Early renal function trajectories, cytomegalovirus serostatus and long-term graft outcomes in kidney transplant recipients
Abstract
Background: Improved recognition of factors influencing graft survival has led to better short-term kidney transplant outcomes. However, efforts to prevent long-term graft decline and improve graft survival have seen more modest improvements. The adoption of electronic health records has enabled better recording and identification of donor-recipient factors through the use of modern statistical techniques. We have previously shown in a prevalent renal transplant population that episodes of rapid deterioration are associated with graft loss.
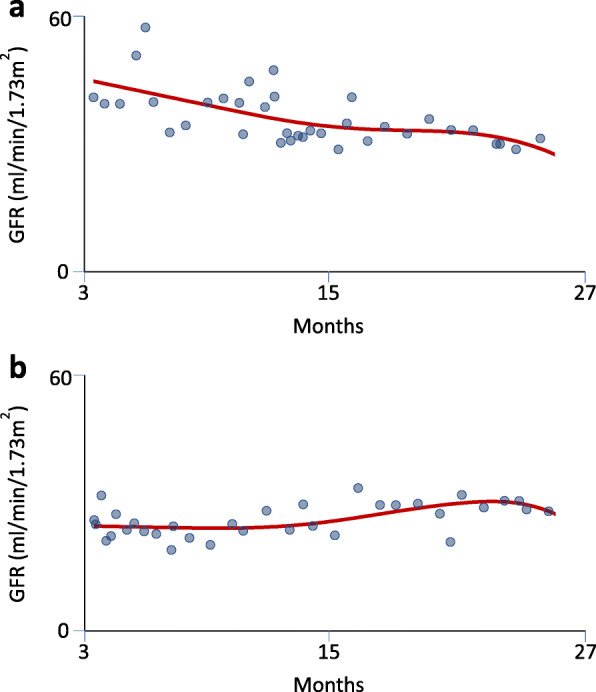
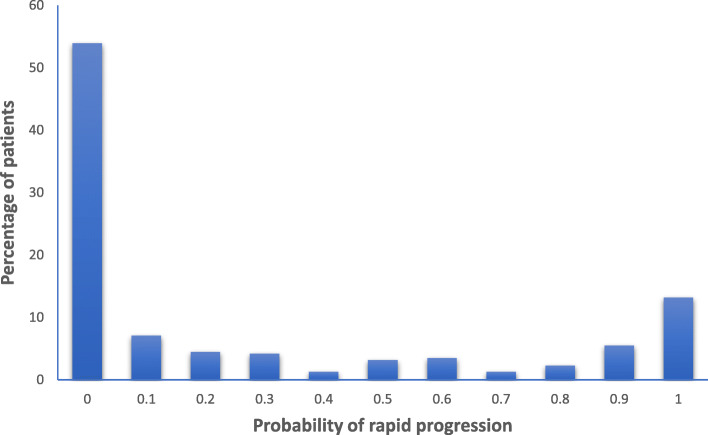
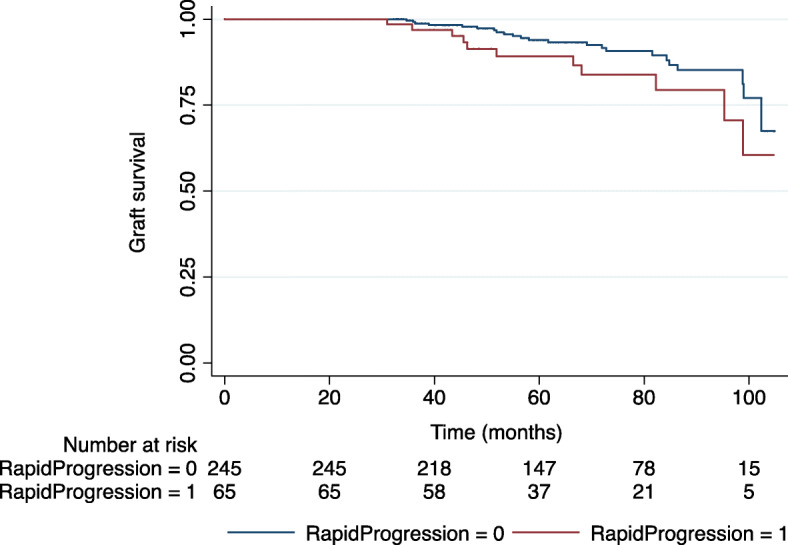
Methods: Estimated glomerular filtration rates (eGFR) between 3 and 27 months after transplantation were collected from 310 kidney transplant recipients. We utilised a Bayesian approach to estimate the most likely eGFR trajectory as a smooth curve from an average of 10,000 Monte Carlo samples. The probability of having an episode of rapid deterioration (decline greater than 5 ml/min/1.73 m2 per year in any 1-month period) was calculated. Graft loss and mortality data was collected over a median follow-up period of 8 years. Factors associated with having an episode of rapid deterioration and associations with long-term graft loss were explored.
Results: In multivariable Cox Proportional Hazard analysis, a probability greater than 0.8 of rapid deterioration was associated with long-term death-censored graft loss (Hazard ratio 2.17; 95% Confidence intervals [CI] 1.04-4.55). In separate multivariable logistic regression models, cytomegalovirus (CMV) serostatus donor positive to recipient positive (Odds ratio [OR] 3.82; 95%CI 1.63-8.97), CMV donor positive (OR 2.06; 95%CI 1.15-3.68), and CMV recipient positive (OR 2.03; 95%CI 1.14-3.60) were associated with having a greater than 0.8 probability of an episode of rapid deterioration.
Conclusions: Early episodes of rapid deterioration are associated with long-term death-censored graft loss and are associated with cytomegalovirus seropositivity. Further study is required to better manage these potentially modifiable risks factors and improve long-term graft survival.
Keywords: Allograft function; Bayesian; Cytomegalovirus serostatus; Estimated glomerular filtration rate; Kidney transplantation.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Impact of Cytomegalovirus Serostatus on Allograft Loss and Mortality Within the First Year After Kidney Transplantation: An Analysis of the National Transplant Registry.Transplant Proc. 2020 Apr;52(3):829-835. doi: 10.1016/j.transproceed.2020.01.028. Epub 2020 Feb 27. Transplant Proc. 2020. PMID: 32113693
-
Cytomegalovirus serostatus pairing and deceased donor kidney transplant outcomes in adult recipients with antiviral prophylaxis.Transplantation. 2010 Nov 27;90(10):1091-8. doi: 10.1097/TP.0b013e3181f7c053. Transplantation. 2010. PMID: 20885340
-
Cytomegalovirus mismatch still negatively affects patient and graft survival in the era of routine prophylactic and preemptive therapy: A paired kidney analysis.Am J Transplant. 2019 Feb;19(2):573-584. doi: 10.1111/ajt.15183. Epub 2018 Dec 14. Am J Transplant. 2019. PMID: 30431703
-
Belatacept for kidney transplant recipients.Cochrane Database Syst Rev. 2014 Nov 24;2014(11):CD010699. doi: 10.1002/14651858.CD010699.pub2. Cochrane Database Syst Rev. 2014. PMID: 25416857 Free PMC article. Review.
-
Discordance in cytomegalovirus viremia in kidney recipients from the same donor is associated with the worst outcomes.Clin Transplant. 2023 Jun;37(6):e14979. doi: 10.1111/ctr.14979. Epub 2023 Mar 26. Clin Transplant. 2023. PMID: 36967240 Review.
Cited by
-
Immunosenescence: an unexplored role in glomerulonephritis.Clin Transl Immunology. 2022 Nov 20;11(11):e1427. doi: 10.1002/cti2.1427. eCollection 2022. Clin Transl Immunology. 2022. PMID: 36420421 Free PMC article. Review.
-
Costs in the Year Following Deceased Donor Kidney Transplantation: Relationships With Renal Function and Graft Failure.Transpl Int. 2022 May 27;35:10422. doi: 10.3389/ti.2022.10422. eCollection 2022. Transpl Int. 2022. PMID: 35692736 Free PMC article.
-
Effect of the Interrelation between CYP3A5 Genotype, Concentration/Dose Ratio and Intrapatient Variability of Tacrolimus on Kidney Graft Function: Monte Carlo Simulation Approach.Pharmaceutics. 2021 Nov 20;13(11):1970. doi: 10.3390/pharmaceutics13111970. Pharmaceutics. 2021. PMID: 34834385 Free PMC article.
-
Stratification of Kidney Transplant Recipients Into Five Subgroups Based on Temporal Disease Trajectories.Transplant Direct. 2024 Jan 24;10(2):e1576. doi: 10.1097/TXD.0000000000001576. eCollection 2024 Feb. Transplant Direct. 2024. PMID: 38274475 Free PMC article.
References
-
- U.S. Renal Data System . USRDS 2012 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. Bethseda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
