

Impact of 18F-FDG PET/CT, CT and EBUS/TBNA on preoperative mediastinal nodal staging of NSCLC
- PMID: 33731050
- PMCID: PMC7967993
- DOI: 10.1186/s12880-021-00580-w
Impact of 18F-FDG PET/CT, CT and EBUS/TBNA on preoperative mediastinal nodal staging of NSCLC
Abstract
Background: Staging of non-small-cell lung cancer (NSCLC) is a multidisciplinary process involving imaging, endoscopic and surgical techniques. This study aims at investigating the diagnostic accuracy of 18F-FDG PET/CT, CT scan, and endobronchial ultrasound/transbronchial needle aspirate (EBUS/TBNA) in preoperative mediastinal lymph nodes (MLNs) staging of NSCLC.
Methods: We identified all patients who were diagnosed with NSCLC at the King Hussein Cancer Center in Amman, Jordan, between July 2011 and December 2017. We collected their relevant clinical, radiological, and histopathological findings. The per-patient analysis was performed on all patients (N = 101) and then on those with histopathological confirmation (N = 57), followed by a per-lymph-node-station basis overall, and then according to distinct N-stage categories.
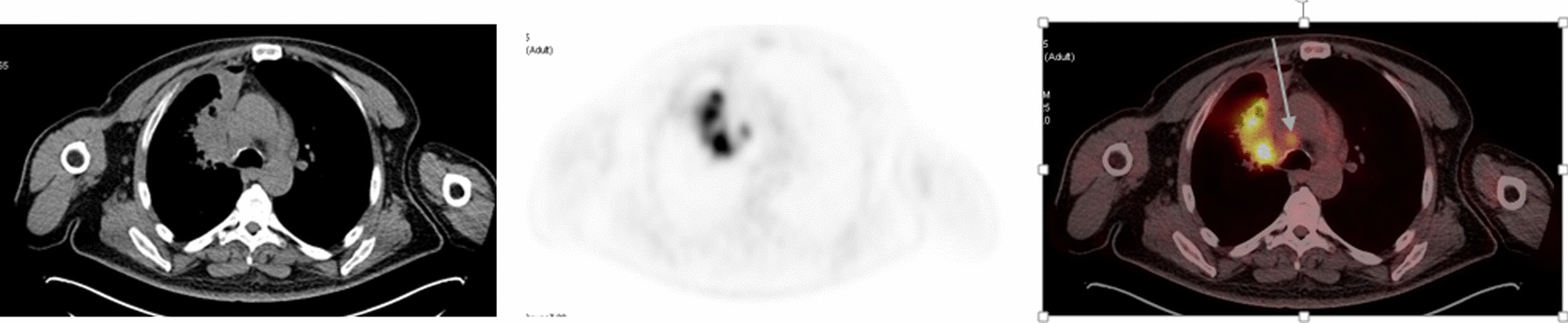
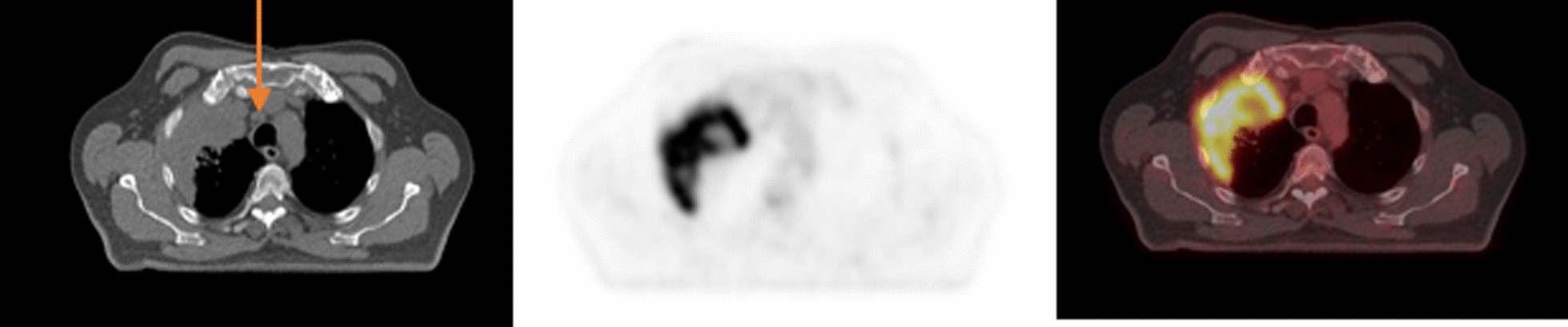
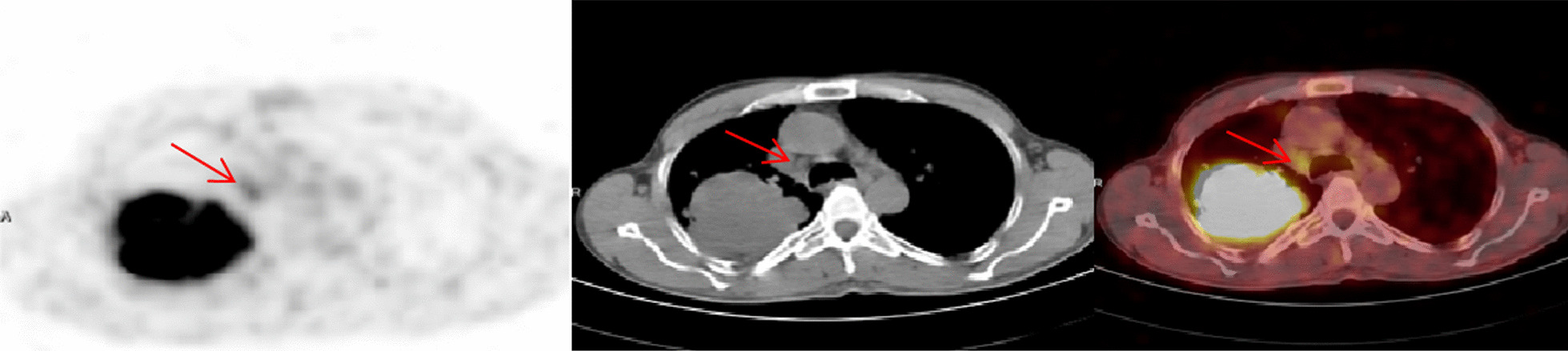
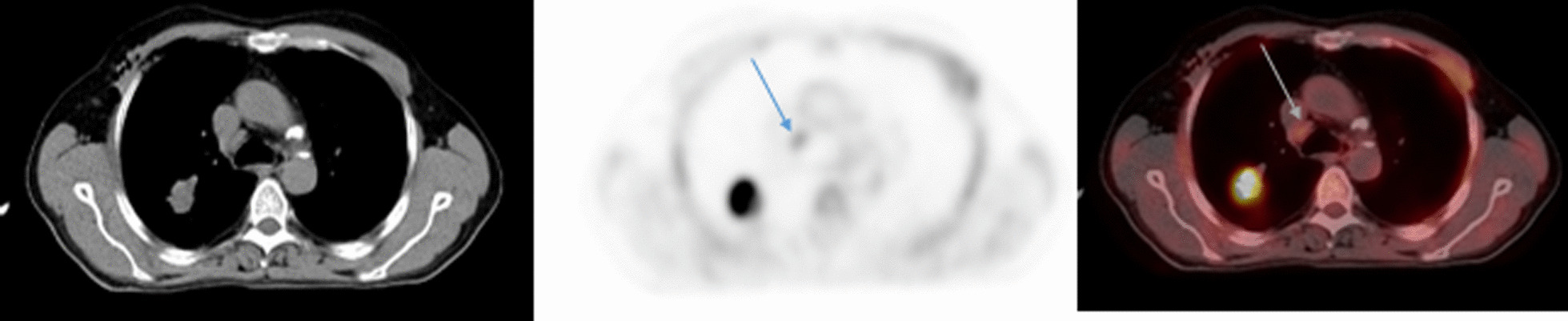
Results: 18F-FDG PET/CT, in comparison to CT, had a better sensitivity (90.5% vs. 75%, p = 0.04) overall and in patients with histopathological confirmation (83.3% vs. 54.6%), and better specificity (60.5% vs. 43.6%, p = 0.01) overall and in patients with histopathological confirmation in MLN staging (60.6% vs. 38.2%). Negative predictive value of mediastinoscopy, EBUS/TBNA, and 18F-FDG PET/CT were (87.1%), (90.91%), and (83.33%) respectively. The overall accuracy was highest for mediastinoscopy (88.6%) and EBUS/TBNA (88.2%), followed by 18F-FDG PET/CT (70.2%). Dividing patients into N1 disease vs. those with N2/N3 disease yielded similar findings. Comparison between 18F-FDG PET/CT and EBUS/TBNA in patients with histopathological confirmation shows 28 correlated true positive and true negative findings with final N-staging. In four patients, 18F-FDG PET/CT detected metastatic MLNs that would have otherwise remained undiscovered by EBUS/TBNA alone. Lymph nodes with a maximal standardized uptake value (SUVmax) more than 3 were significantly more likely to be true-positive.
Conclusion: Multimodality staging of the MLNs in NSCLC is essential to provide accurate staging and the appropriate treatment. 18F-FDG PET/CT has better overall diagnostic utility when compared to the CT scan. The NPV of 18F-FDG PET/CT in MLNs is reliable and comparable to the NPV of EBUS/TBNA. SUVmax of MLNs can help in predicting metastases, but nevertheless, a positive 18F-FDG PET/CT MLNs particularly if such a result would change the treatment plan, should be verified histopathologically.
Keywords: 18F-FDG PET/CT; EBUS/TBNA; Mediastinal lymph node staging; NPV; NSCLC.
Conflict of interest statement
Akram Al-Ibraheem, Nader Hirmas, Stefano Fanti, Diana Paez, Fawzi Abuhijla, Dalia Al-Rimawi, Ula Al-Rasheed, Riad Abdeijalil, Feras Hawari, Kamal Alrabi and Asem Mansour declare they have no conflict of interest relevant to this research.
Figures
Similar articles
-
Is FDG-PET/CT used correctly in the combined approach for nodal staging in NSCLC patients?Niger J Clin Pract. 2020 Jun;23(6):842-847. doi: 10.4103/njcp.njcp_2_19. Niger J Clin Pract. 2020. PMID: 32525121
-
Systematic Compared With Targeted Staging With Endobronchial Ultrasound in Patients With Lung Cancer.Ann Thorac Surg. 2018 Aug;106(2):398-403. doi: 10.1016/j.athoracsur.2018.02.088. Epub 2018 Apr 6. Ann Thorac Surg. 2018. PMID: 29630875
-
Is it necessary to sample the contralateral nodal stations by EBUS-TBNA in patients with lung cancer and clinical N0 / N1 on PET-CT?Lung Cancer. 2020 Apr;142:9-12. doi: 10.1016/j.lungcan.2020.01.014. Epub 2020 Jan 13. Lung Cancer. 2020. PMID: 32062200
-
PET-CT for assessing mediastinal lymph node involvement in patients with suspected resectable non-small cell lung cancer.Cochrane Database Syst Rev. 2014 Nov 13;2014(11):CD009519. doi: 10.1002/14651858.CD009519.pub2. Cochrane Database Syst Rev. 2014. PMID: 25393718 Free PMC article. Review.
-
Endobronchial ultrasound-guided transbronchial needle aspiration for non-small cell lung cancer staging.Am J Respir Crit Care Med. 2014 Mar 15;189(6):640-9. doi: 10.1164/rccm.201311-2007CI. Am J Respir Crit Care Med. 2014. PMID: 24484269 Review.
Cited by
-
The Diagnostic Value of Endobronchial Ultrasound-Guided Fine Needle Aspiration (EBUS-FNA) in Diagnosing FDG-PET-Avid Lymph Nodes in Extrapulmonary Malignancies.Cureus. 2024 Aug 31;16(8):e68269. doi: 10.7759/cureus.68269. eCollection 2024 Aug. Cureus. 2024. PMID: 39350840 Free PMC article.
-
The impact of staging FDG-PET/CT on treatment for stage III NSCLC - an analysis of population-based data from Ontario, Canada.Front Oncol. 2023 Aug 23;13:1210945. doi: 10.3389/fonc.2023.1210945. eCollection 2023. Front Oncol. 2023. PMID: 37681028 Free PMC article.
-
Endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing thoracic lesions: a retrospective cohort study.Front Med (Lausanne). 2024 May 10;11:1383600. doi: 10.3389/fmed.2024.1383600. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38799146 Free PMC article.
-
Canadian Consensus Recommendations for the Management of Operable Stage II/III Non-Small-Cell Lung Cancer: Results of a Modified Delphi Process.Curr Oncol. 2023 Dec 6;30(12):10363-10384. doi: 10.3390/curroncol30120755. Curr Oncol. 2023. PMID: 38132389 Free PMC article.
-
A Nomogram to Predict Benign/Malignant Mediastinal Lymph Nodes Based on EBUS Sonographic Features.Int J Clin Pract. 2024 Feb 29;2024:3711123. doi: 10.1155/2024/3711123. eCollection 2024. Int J Clin Pract. 2024. PMID: 38454935 Free PMC article.
References
-
- Zhang Y, Elam Y, Hall P, Williams H, Pucar D, Patel V. The role of fluorodeoxy-D-glucose positron emission tomography/computed tomography in nodal staging of nonsmall cell lung cancer in sequential surgical algorithm. World J Nucl Med. 2017;16(4):281–285. doi: 10.4103/1450-1147.215486. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
