

Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options
- PMID: 33720773
- PMCID: PMC7969169
- DOI: 10.1161/CIRCULATIONAHA.120.050686
Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options
Abstract
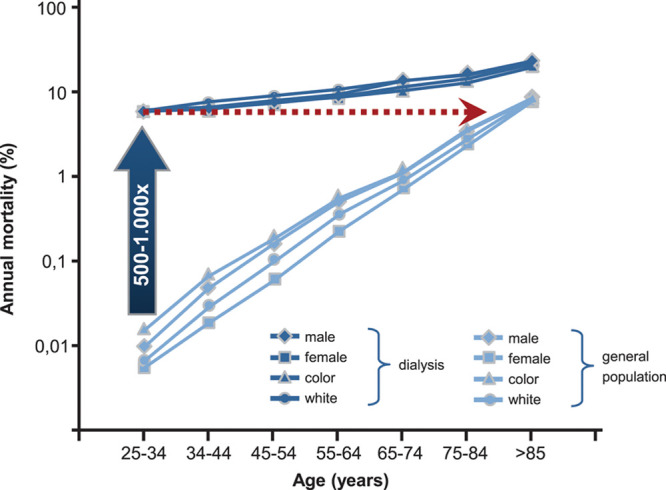
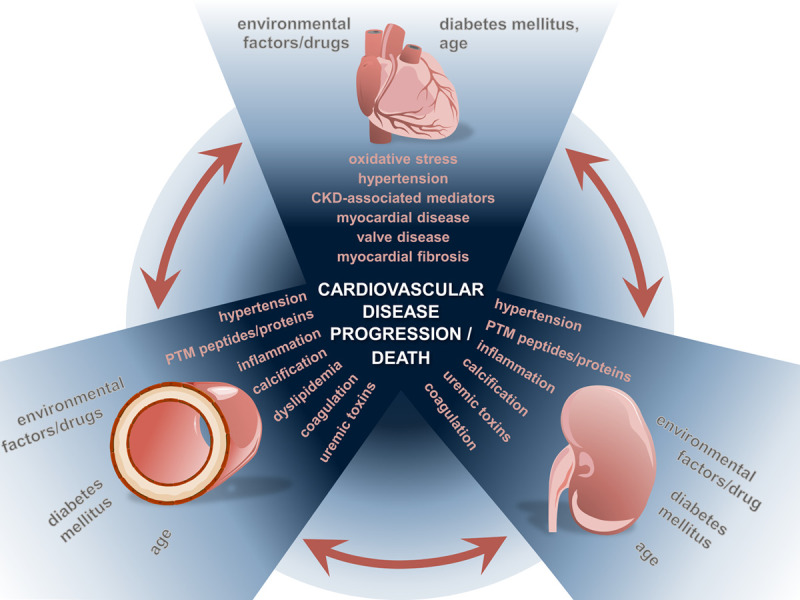
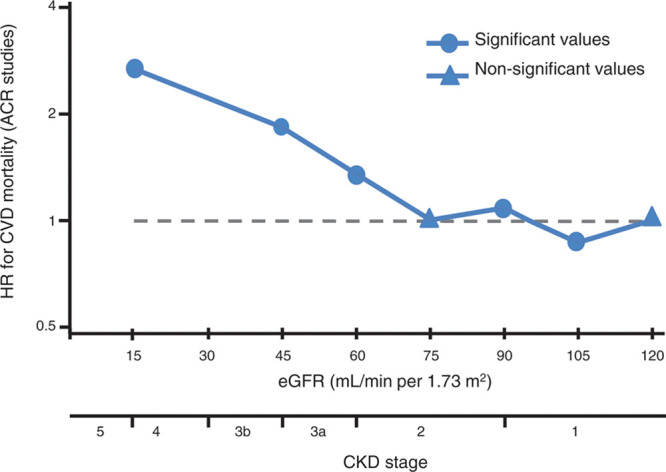
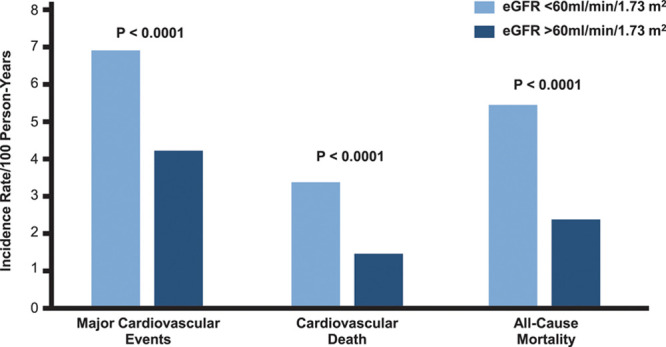
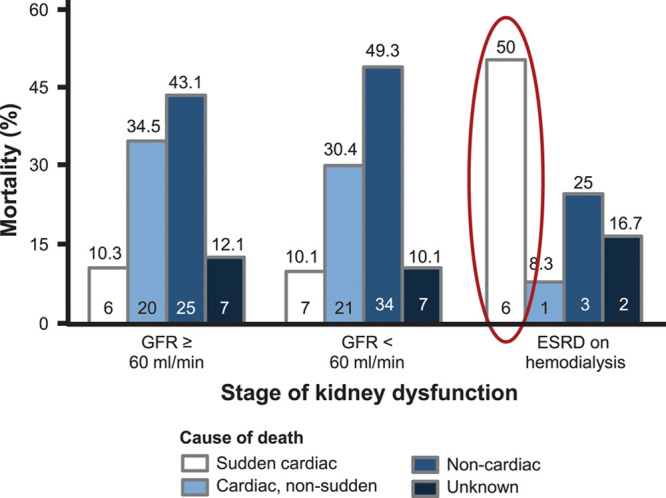
Patients with chronic kidney disease (CKD) exhibit an elevated cardiovascular risk manifesting as coronary artery disease, heart failure, arrhythmias, and sudden cardiac death. Although the incidence and prevalence of cardiovascular events is already significantly higher in patients with early CKD stages (CKD stages 1-3) compared with the general population, patients with advanced CKD stages (CKD stages 4-5) exhibit a markedly elevated risk. Cardiovascular rather than end-stage kidney disease (CKD stage 5) is the leading cause of death in this high-risk population. CKD causes a systemic, chronic proinflammatory state contributing to vascular and myocardial remodeling processes resulting in atherosclerotic lesions, vascular calcification, and vascular senescence as well as myocardial fibrosis and calcification of cardiac valves. In this respect, CKD mimics an accelerated aging of the cardiovascular system. This overview article summarizes the current understanding and clinical consequences of cardiovascular disease in CKD.
Keywords: arrhythmias; cardiovascular disease; chronic kidney disease; clinical aspects; death; heart failure; sudden cardiac.
Figures
Similar articles
-
Cardiovascular complications in chronic kidney disease: a review from the European Renal and Cardiovascular Medicine Working Group of the European Renal Association.Cardiovasc Res. 2023 Sep 5;119(11):2017-2032. doi: 10.1093/cvr/cvad083. Cardiovasc Res. 2023. PMID: 37249051 Free PMC article. Review.
-
Serum Calcification Propensity and Clinical Events in CKD.Clin J Am Soc Nephrol. 2019 Nov 7;14(11):1562-1571. doi: 10.2215/CJN.04710419. Epub 2019 Oct 28. Clin J Am Soc Nephrol. 2019. PMID: 31658949 Free PMC article.
-
Endothelium-Dependent and -Independent Vascular Function in Advanced Chronic Kidney Disease.Clin J Am Soc Nephrol. 2017 Oct 6;12(10):1588-1594. doi: 10.2215/CJN.12811216. Epub 2017 Aug 7. Clin J Am Soc Nephrol. 2017. PMID: 28784655 Free PMC article.
-
Coronary flow reserve is predictive of the risk of cardiovascular death regardless of chronic kidney disease stage.Kidney Int. 2018 Feb;93(2):501-509. doi: 10.1016/j.kint.2017.07.025. Epub 2017 Oct 13. Kidney Int. 2018. PMID: 29032954 Free PMC article.
-
The Cardio-Kidney Patient: Epidemiology, Clinical Characteristics and Therapy.Circ Res. 2023 Apr 14;132(8):902-914. doi: 10.1161/CIRCRESAHA.122.321748. Epub 2023 Apr 13. Circ Res. 2023. PMID: 37053284 Free PMC article. Review.
Cited by
-
Non-High-Density Lipoprotein Cholesterol and Cardiovascular Outcomes in Chronic Kidney Disease: Results from KNOW-CKD Study.Nutrients. 2022 Sep 14;14(18):3792. doi: 10.3390/nu14183792. Nutrients. 2022. PMID: 36145167 Free PMC article.
-
Protection against Incidences of Serious Cardiovascular Events Study with daily fish oil supplementation in dialysis patients (PISCES): protocol for a randomised controlled trial.BMJ Open. 2024 Jan 10;14(1):e072239. doi: 10.1136/bmjopen-2023-072239. BMJ Open. 2024. PMID: 38199618 Free PMC article.
-
Sarcopenia and cardiovascular disease in patients with and without kidney disease: what do we know?Int Urol Nephrol. 2023 May;55(5):1161-1171. doi: 10.1007/s11255-022-03393-0. Epub 2022 Nov 3. Int Urol Nephrol. 2023. PMID: 36327007 Review.
-
Relationship between Serum Indoxyl Sulfate and Klotho Protein and Vascular Calcification in Patients with Chronic Kidney Disease Stages 3-5.Int J Endocrinol. 2024 Feb 14;2024:8229604. doi: 10.1155/2024/8229604. eCollection 2024. Int J Endocrinol. 2024. PMID: 38385060 Free PMC article.
-
Clonal hematopoiesis, somatic mosaicism, and age-associated disease.Physiol Rev. 2023 Jan 1;103(1):649-716. doi: 10.1152/physrev.00004.2022. Epub 2022 Sep 1. Physiol Rev. 2023. PMID: 36049115 Free PMC article. Review.
References
-
- Stevens PE, O’Donoghue DJ, de Lusignan S, Van Vlymen J, Klebe B, Middleton R, Hague N, New J, Farmer CK. Chronic kidney disease management in the United Kingdom: NEOERICA project results. Kidney Int. 2007;72:92–99. doi: 10.1038/sj.ki.5002273 - PubMed
-
- Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. Lancet. 2017;389:1238–1252. doi: 10.1016/S0140-6736(16)32064-5 - PubMed
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;325 suppl 3S112–S119. doi: 10.1053/ajkd.1998.v32.pm9820470 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
